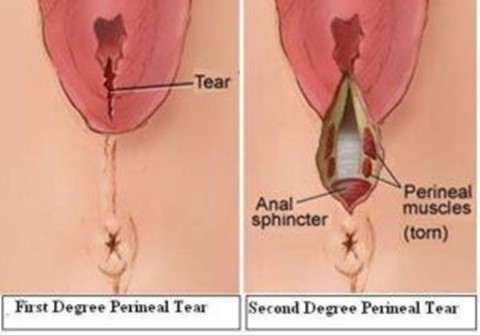
A nurse is reinforcing teaching about reducing the risk of perineal infection with a client who had a vaginal birth. Which of the following information should the nurse include in the teaching? (Select all that apply.)
Apply ice packs to the perineal area several times daily.
Sit on an inflatable donut to protect the perineum.
Perform hand hygiene before and after voiding.
Blot the perineal area dry after voiding.
Clean the perineal area from front to back.
Correct Answer : C,D,E
Choice A reason: While ice packs can help reduce swelling and discomfort, they are not essential for preventing infection.
Choice B reason: Sit on an inflatable donut to protect the perineum is incorrect, as this can increase pressure and blood flow to the perineum and delay healing. The nurse should advise the client to avoid sitting on hard or uneven surfaces and to use a pillow or a cushion for comfort.
Choice C reason: Perform hand hygiene before and after voiding is correct, as this can prevent contamination and infection of the perineal area. The nurse should instruct the client to wash their hands with soap and water or use an alcohol-based hand sanitizer before and after using the toilet.
Choice D reason: Blot the perineal area dry after voiding is correct, as this can keep the perineal area clean and dry and prevent irritation and infection. The nurse should instruct the client to use a clean, soft cloth or tissue and gently pat or blot the perineal area from front to back after voiding.
Choice E reason: Clean the perineal area from front to back is correct, as this can prevent bacteria from entering the vagina or urethra and causing infection. The nurse should instruct the client to use a peri-botle filled with warm water and squirt it over the perineal area from front to back after each voiding or bowel movement. The client should also change their perineal pad frequently and dispose of it properly.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Position the client on her side is correct, as this is the first action the nurse should take according to the ABCDE priority framework. Late decelerations are symmetrical decreases in the fetal heart rate that begin after the peak of the contraction and return to baseline after the contraction ends, which indicate uteroplacental insufficiency and fetal hypoxia. Positioning the client on her side can improve blood flow and oxygen delivery to the placenta and fetus by relieving pressure on the vena cava and aorta.
Choice B reason: Elevate the client's legs is incorrect, as this is not a priority action for a client who has late decelerations. Elevating the legs can increase venous return and cardiac output, but it can also reduce blood flow and oxygen delivery to the placenta and fetus by compressing the vena cava and aorta.
Choice C reason: Administer oxygen via face mask is incorrect, as this is not the first action the nurse should take, although it is important to do later. Administering oxygen can increase oxygen saturation and delivery to the placenta and fetus, but it does not address the cause of uteroplacental insufficiency or improve blood flow.
Choice D reason: Increase the infusion rate of the IV fluid is incorrect, as this is not the first action the nurse should take, although it may be indicated later. Increasing the infusion rate of IV fluid can expand blood volume and improve placental perfusion, but it does not address the cause of uteroplacental insufficiency or improve blood flow. The nurse should obtain a provider's order before increasing the IV fluid rate.
Correct Answer is B
Explanation
Choice A reason:
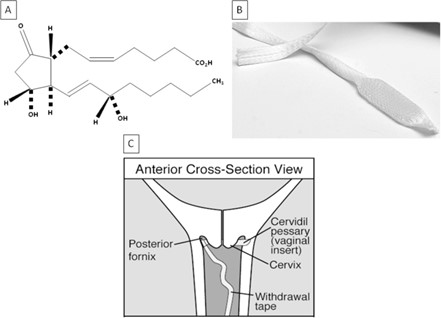
Dinoprostone stimulates uterine contractions is incorrect, as this is not the primary purpose of the medication. Dinoprostone is a prostaglandin that can induce labor by ripening the cervix and enhancing uterine contractility, but it is not used solely for stimulating contractions.
Choice B reason:
Dinoprostone promotes softening of the cervix is correct, as this is the main purpose of the medication. Dinoprostone is used to prepare the cervix for labor by increasing its softness, dilation, and effacement. This can facilitate the descent of the fetus and shorten the duration of labor.
Choice C reason:
Dinoprostone relaxes uterine contractions is incorrect, as this is the opposite effect of the medication. Dinoprostone can increase uterine tone and frequency, which can help initiate or augment labor. The nurse should monitor the client for signs of uterine hyperstimulation or fetal distress.
Choice D reason:
Dinoprostone assists with ending the pregnancy is incorrect, as this is not the intended use of the medication. Dinoprostone can be used to terminate a pregnancy in some cases, such as fetal demise or missed abortion, but it is not routinely used for this purpose. The nurse should explain to the client that dinoprostone is used to induce labor and not to end a pregnancy.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today