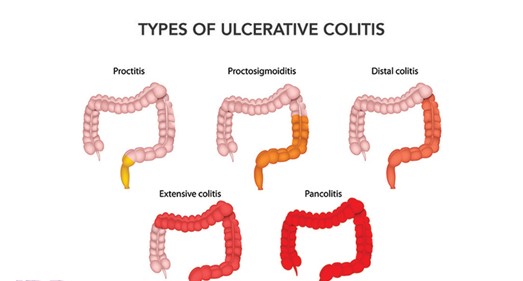
A nurse is caring for a client who has ulcerative colitis and is teaching the client about the common link with Crohn's disease. Which of the following information should the nurse include?
Both are inflammatory.
Both affect the entire alimentary canal.
Both will require a bowel diversion.
Both disorders are caused by low-fat, high-fiber diets.
The Correct Answer is A
Choice A reason: This is the correct answer because both ulcerative colitis and Crohn's disease are inflammatory bowel diseases (IBD) that cause chronic inflammation of the digestive tract. The inflammation can cause symptoms such as abdominal pain, diarrhea, bleeding, weight loss, or fever. The nurse should educate the client on how to manage inflammation and prevent complications.
Choice B reason: This is incorrect because both ulcerative colitis and Crohn's disease do not affect the entire alimentary canal, but different parts of it. Ulcerative colitis affects only the colon (large intestine) and rectum, while Crohn's disease can affect any part of the digestive tract from mouth to anus, most commonly the ileum (the last part of the small intestine). The nurse should explain the differences in location and extent of
the diseases.
Choice C reason: This is incorrect because both ulcerative colitis and Crohn's disease do not always require a bowel diversion, but only in some cases. A bowel diversion is a surgical procedure that creates an opening (stoma) in the abdomen to divert fecal matter into an external bag or pouch. It may be done to treat severe complications such as perforation, obstruction, fistula, or cancer. The nurse should inform the client about the indications, types, and care of bowel diversions.
Choice D reason: This is incorrect because both ulcerative colitis and Crohn's disease are not caused by low-fat, high-fiber diets, but by unknown factors. The exact causes of IBD are not clear, but they may involve genetic, immune, environmental, or microbial factors. Low-fat, high-fiber diets may help prevent or reduce symptoms of IBD, but they do not cause them. The nurse should advise the client on how to follow a balanced and nutritious diet that suits their individual needs and preferences.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A Reason: A virus is not detected by the KOH test, which is used to diagnose fungal infections of the skin, hair, or nails. A virus can be detected by other tests, such as polymerase chain reaction (PCR) or viral culture.
Choice B Reason: A fungal infection is detected by the KOH test, which dissolves the skin cells and leaves behind the fungal elements that can be seen under a microscope. A fungal infection can cause symptoms such as itching, scaling, redness, or blisters.
Choice C Reason: A bacterial infection is not detected by the KOH test, which is specific for fungi. A bacterial infection can be detected by other tests, such as gram stain or culture.
Choice D Reason: Cancer is not detected by the KOH test, which is not a screening tool for malignancy. Cancer can be detected by other tests, such as biopsy or imaging.
Correct Answer is ["D","E"]
Explanation
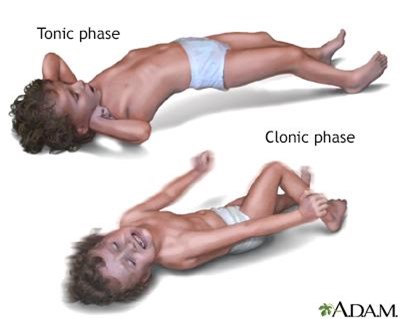
Choice A Reason: This choice is incorrect. Placing the client into a supine position is not an action that the nurse should take, as it can compromise the airway and increase the risk of aspiration. The nurse should position the client on their side with their head tilted slightly forward to allow saliva and secretions to drain out of their mouth.
Choice B Reason: This choice is incorrect. Applying restraints is not an action that the nurse should take, as it can cause injury and increase agitation. The nurse should protect the client from harm by removing any objects or furniture that may cause harm and padding any hard surfaces with blankets or pillows.
Choice C Reason: This choice is incorrect. Inserting a bite stick into the client's mouth is not an action that the nurse should take, as it can cause injury and obstruction. The nurse should never force anything into the client's mouth during a seizure, as it can damage their teeth, gums, tongue, or jaw.
Choice D Reason: This is a correct choice. Loosening restrictive clothing is an action that the nurse should take, as it can improve breathing and circulation. The nurse should unbutton any tight collars, belts, or ties that may constrict the chest or neck.
Choice E Reason: This is a correct choice. Placing a pillow under the client's head is an action that the nurse should take, as it can prevent injury and provide comfort. The nurse should support the client's head with a soft pillow or cushion to prevent hitting it against any hard surfaces.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today