A nurse is caring for a client who is 4 hr postpartum. The nurse finds a small amount of lochia rubra on the client's perineal pad. The fundus is midline and firm at the umbilicus. Which of the following actions should the nurse take?
Increase the rate of IV fluids.
Assist the client to ambulate.
Perform fundal massage.
Check for blood under the client's buttock.
The Correct Answer is D
Check for blood under the client's buttock. This is because lochia rubra is the normal vaginal discharge that occurs after childbirth, consisting of blood, mucus, and tissue from the placenta and the uterus lining. It is usually heavy for the first three to four days and can pool under the client's buttocks if they are lying down. Checking for blood under the buttock can help assess the amount of bleeding and prevent complications such as infection or hemorrhage.
The other choices are not correct for the following reasons:
A. Increasing the rate of the IV fluids is not necessary because the client's fundus is firm and midline, indicating that the uterus is contracting well and preventing excessive bleeding.
B. Assisting the client to ambulate is not advisable because it can increase the lochia flow and cause fainting or dizziness due to blood loss.
C. Performing fundal massage is not indicated because the fundus is already firm and midline, meaning that the uterus is adequately contracted. Massaging a firm fundus can cause pain and discomfort to the client.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Endometritis. This is because the client's symptoms suggest that she has endometritis, which is an infection of the lining of the uterus. Endometritis is a common postpartum complication that can occur after vaginal or cesarean delivery. The client may also have foul-smelling vaginal discharge, chills, and fatigue.
Choice B is wrong because cystitis is an infection of the bladder that causes pain or burning during urination, not cramping.
Choice C is wrong because dehydration does not cause fever or persistent cramping.
Choice D is wrong because hypovolemic shock is a condition of low blood volume that causes low blood pressure, rapid pulse, and pale skin, not fever or cramping.
Correct Answer is D
Explanation
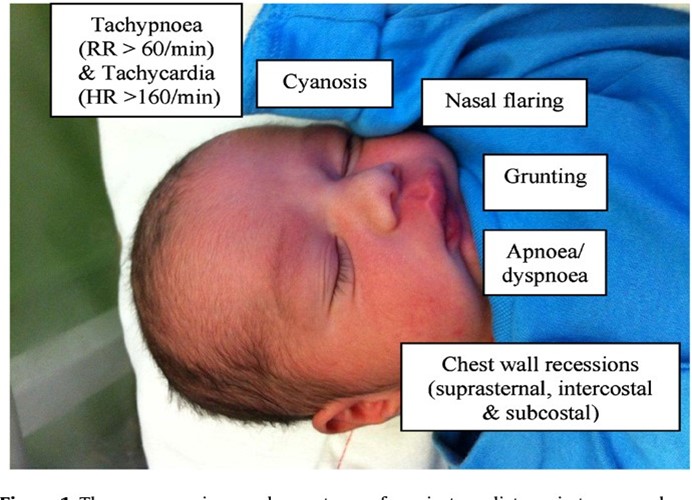
Sternal or chest retractions. This is because sternal or chest retractions are a sign of respiratory distress in newborns, which means they are having difficulty breathing. Chest retractions occur when the baby's chest pulls in with each breath, indicating that they are using extra muscles to breathe. This can be caused by various conditions that affect the lungs, such as respiratory distress syndrome (RDS), transient tachypnea of the newborn (TTN), meconium aspiration syndrome (MAS), pneumonia, or congenital heart defects.
 Choice A is not correct because mucus draining from the nose is not a symptom of respiratory distress in newborns. It is normal for newborns to have some mucus in their nose and mouth after birth, which can be cleared by suctioning or wiping.
Choice A is not correct because mucus draining from the nose is not a symptom of respiratory distress in newborns. It is normal for newborns to have some mucus in their nose and mouth after birth, which can be cleared by suctioning or wiping.
Mucus drainage does not interfere with breathing unless it is excessive or thick.
Choice B is not correct because cyanosis of the hands and feet is not a symptom of respiratory distress in newborns. It is normal for newborns to have bluish discoloration of their hands and feet, called acrocyanosis, for the first few days after birth. This is due to immature circulation and does not indicate a lack of oxygen. Cyanosis of the central parts of the body, such as the face, lips, and tongue, is more concerning and should be reported.
Choice C is not correct because irregular heart rate is not a symptom of respiratory distress in newborns. It is normal for newborns to have some variations in their heart rate, especially during sleep cycles. The normal heart rate range for newborns is 100 to 160 beats per minute. A heart rate that is too fast (tachycardia) or too slow (bradycardia) may indicate a problem with the heart or other organs³.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today