A nurse is caring for a patient who is 8 days post-abdominal surgery and reports sudden discomfort at the incision site. Upon examination, the nurse notices the wound edges are partially separated with serosanguineous drainage present. What is the most appropriate initial nursing action?
Apply a dry sterile dressing to the wound.
Apply an antibiotic ointment directly to the open wound.
Notify the healthcare provider immediately.
Encourage the patient to ambulate to improve circulation.
The Correct Answer is C
A. Apply a dry sterile dressing to the wound: While a dressing is needed, a dry dressing can adhere to the exposed tissues. The wound should be covered with a moist, sterile dressing to protect the open tissue.
B. Apply an antibiotic ointment directly to the open wound: Dehiscence is a mechanical failure, not an infection (at this stage). Topical antibiotics are not the initial priority and may irritate the wound.
C. Notify the healthcare provider immediately: This is the most appropriate initial nursing action. Wound dehiscence is a serious surgical complication that requires prompt evaluation by the surgeon. The nurse must immediately stabilize the patient and the wound and communicate the critical finding to the provider for repair or management planning.
D. Encourage the patient to ambulate to improve circulation: Ambulation, physical exertion, or straining (e.g., coughing, bending) could further separate the wound edges, potentially leading to a much more severe evisceration. The patient should be kept calm and placed in a position to minimize tension on the wound.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
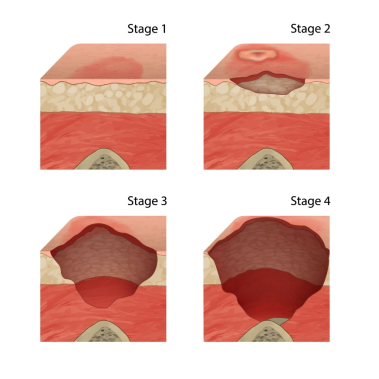
A. Stage 3 pressure injury: A Stage 3 injury involves full-thickness skin loss, extending into the subcutaneous fat.
B. Unstageable pressure injury: An Unstageable injury requires the base of the wound to be obscured by slough or eschar. This wound is visible as a blister/open ulcer.
C. Stage 2 pressure injury: A Stage 2 pressure injury is defined as partial-thickness loss of skin involving the epidermis and/or dermis. It presents as a shallow open ulcer with a red-pink wound bed, or an intact or ruptured serum-filled blister.
D. Stage 1 pressure injury: A Stage 1 injury involves intact skin with nonblanchable redness.
Correct Answer is B
Explanation
A. A patient with adequate hydration and skin care regimen.Adequate hydration and a good skin care regimen are preventive measures that significantly decrease the risk of developing a pressure injury.
B. An immobile patient with poor nutritional status.Immobility (prolonged, unrelieved pressure and shear) is the primary mechanical cause of pressure injuries. Poor nutritional status (specifically, low protein and poor hydration) compromises the integrity of the skin and the body's ability to repair tissue, drastically multiplying the overall risk.
C. A mobile patient with a history of diabetes.While diabetes is a risk factor due to poor circulation and neuropathy, a mobile patient can independently relieve pressure, which is the most critical factor in prevention. Therefore, they are at a lower risk than an immobile patient.
D. A patient who regularly changes position every hour.Regular repositioning (typically every two hours in bed, or more frequently in a chair) is the single most effective intervention for preventing pressure injuries. This patient is actively mitigating their risk.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today