A nurse is caring for an infant who has gastroesophageal reflux (GER). Which of the following actions should the nurse take to prevent regurgitation? (Select all that apply.)
Thicken the infant's formula with cereal.
Avoid giving the infant citrus juices.
Position the child with their head elevated after meals.
Place the infant's head on a soft pillow while sleeping.
Administer an antiemetic to the infant.
Correct Answer : A,B,C
A. Thicken the infant's formula with cereal: Thickening the infant's formula with cereal can help reduce the likelihood of regurgitation by increasing its viscosity and promoting better gastric emptying. This can help decrease the frequency and severity of gastroesophageal reflux episodes.
B. Avoid giving the infant citrus juices: Citrus juices are acidic and can exacerbate gastroesophageal reflux symptoms in infants. Avoiding citrus juices can help reduce the acidity of the stomach contents, potentially decreasing the likelihood of regurgitation.
C. Position the child with their head elevated after meals: Keeping the infant in an upright position with the head elevated after meals can help prevent regurgitation by reducing the likelihood of gastric contents flowing back into the esophagus. This position facilitates gravity-assisted digestion and minimizes pressure on the lower esophageal sphincter.
D. Place the infant's head on a soft pillow while sleeping: Placing the infant's head on a soft pillow while sleeping is not recommended as it increases the risk of suffocation and sudden infant death syndrome (SIDS). Infants should always be placed on their back to sleep in a flat, firm surface without pillows or soft bedding to reduce the risk of adverse events.
E. Administer an antiemetic to the infant: Administering an antiemetic to the infant is not typically indicated for the management of gastroesophageal reflux in infants, especially as a preventive measure. Antiemetics may have potential side effects and should only be used under the guidance of a healthcare provider for specific indications.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
A. Coarctation of the aorta
Coarctation of the aorta involves a narrowing of the aorta, leading to decreased blood flow to the lower body. It is not associated with increased pulmonary blood flow.
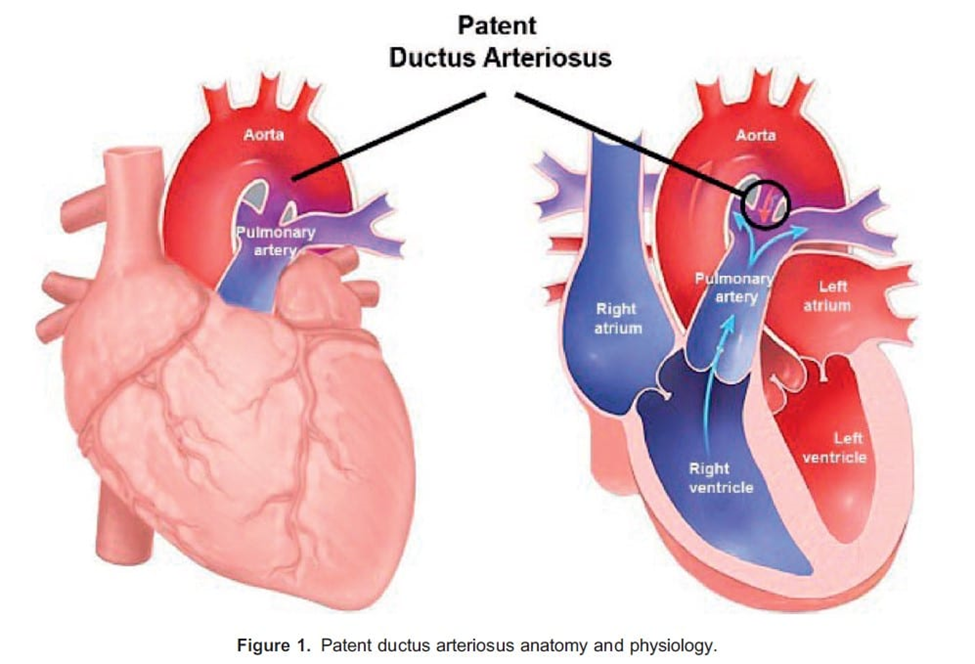
B. Patent ductus arteriosus
Patent ductus arteriosus (PDA) is a congenital heart defect where the ductus arteriosus, a fetal blood vessel that usually closes shortly after birth, remains open. This allows blood to flow from the aorta into the pulmonary artery, increasing pulmonary blood flow. Therefore, option B is correct.
C. Tetralogy of Fallot
Tetralogy of Fallot is a congenital heart defect characterized by four abnormalities, including a ventricular septal defect (VSD), pulmonary stenosis, right ventricular hypertrophy, and an overriding aorta. While it can lead to cyanosis due to right-to-left shunting, it is not primarily associated with increased pulmonary blood flow.
D. Tricuspid atresia
Tricuspid atresia involves the absence of the tricuspid valve, leading to a lack of direct blood flow from the right atrium to the right ventricle. It usually presents with decreased pulmonary blood flow rather than increased pulmonary blood flow.
Correct Answer is A
Explanation
A. Measuring the child's abdominal circumference:
This is the correct action. Assessing the child's abdominal circumference is essential in monitoring the size of the Wilms' tumor and evaluating for any signs of abdominal distention or growth. Changes in abdominal circumference can provide valuable information about the progression of the tumor and any potential complications.
B. Palpating the child's abdomen:
Palpating the child's abdomen is an essential part of the physical examination to assess for the presence of a mass or any tenderness. However, in the case of a child with a known Wilms' tumor, palpation should be performed gently to avoid causing discomfort or disturbing the tumor.
C. Providing clear liquids up to 1 hr prior to surgery:
Providing clear liquids up to 1 hour prior to surgery is not appropriate for a child undergoing surgery, especially if anesthesia is involved. Preoperative fasting guidelines typically require clear liquids to be stopped a few hours before surgery to reduce the risk of aspiration.
D. Continuously monitoring the child's oxygen saturation:
Continuous monitoring of the child's oxygen saturation is an essential aspect of perioperative care, but it is not specific to the preoperative assessment for a child with Wilms' tumor. Oxygen saturation monitoring is typically performed throughout the perioperative period to ensure adequate oxygenation during surgery and recovery.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today