A nurse is collecting data from a client who is at 29 weeks of gestation.
Which of the following findings should the nurse identify as a potential indication of a prenatal complication?
Leg cramps.
Ptyalism.
Blurred vision.
Melasma.
The Correct Answer is C
This can be a sign of preeclampsia, a serious complication of pregnancy that causes high blood pressure and proteinuria.
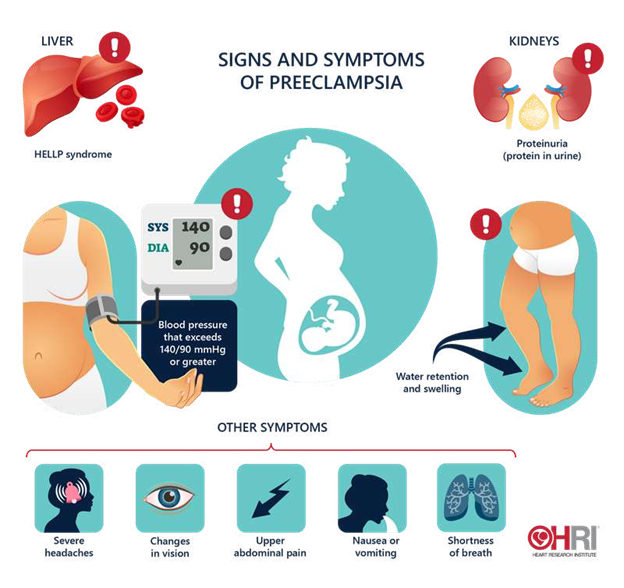
The nurse should report this finding to the provider and monitor the client’s blood pressure, urine protein, and reflexes.
Choice A is wrong because leg cramps are a common discomfort during pregnancy and are not usually a sign of a complication.
Choice B is wrong because ptyalism, or excessive salivation, is a normal physiological change during pregnancy and does not indicate a problem.
Choice D is wrong because melasma, or darkening of the skin on the face, is also a normal physiological change during pregnancy and does not pose a risk to the mother or the fetus.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Contact information for a community mental health center. A community mental health center can provide ongoing outpatient care and support services for a client who has schizophrenia after discharge from an inpatient unit. A community mental health center can also help the client access other resources such as medication, housing, and vocational training.
Choice B is wrong because a list of primary prevention activities is not relevant for a client who already has schizophrenia. Primary prevention aims to prevent the occurrence of a disease or disorder in the first place.
Choice C is wrong because contact information for enrollment in a 12-step program is not appropriate for a client who has schizophrenia unless they also have a substance use disorder. A 12-step program is a self-help group that follows a set of principles to achieve and maintain sobriety.
Choice D is wrong because a referral for respite care services is not necessary for a client who has schizophrenia unless they also have a caregiver who needs temporary relief from their caregiving duties. Respite care services provide short-term care for clients who are dependent on others for their daily needs.
Correct Answer is C
Explanation
A. Keeping a voiding diary can help assess patterns, but it is not the primary instruction when reinforcing an active bladder-training schedule.
B. Drinking 4 liters of fluid is excessive and can worsen urinary frequency and urgency.
C. Voiding every 2 hours while awake is a standard initial bladder-training strategy. It establishes a scheduled pattern and helps prevent episodes of incontinence, with intervals gradually increased as control improves.
D. Eliminating caffeine helps reduce bladder irritation, but it is an adjunct lifestyle modification rather than the core bladder-training technique.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today