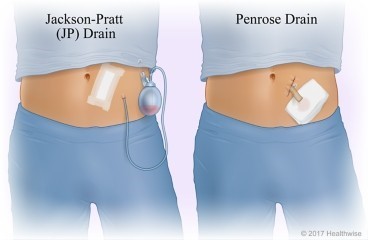
A nurse is completing a dressing change on a client who has a surgical wound drain. Which of the following actions should the nurse take?
Use a separate, sterile swab for each stroke when cleaning the wound.
First clean the drain site and then clean the incision.
Don clean gloves before cleaning the wound.
Cut a 4 x 4 piece of gauze to place around the drain site.
The Correct Answer is A
When completing a dressing change on a client who has a surgical wound drain, the nurse should use a separate, sterile swab for each stroke when cleaning the wound. This helps to prevent the spread of infection and ensures that the wound is properly cleaned.
Option b is incorrect because the nurse should first clean the incision and then clean the drain site.
Option c is incorrect because the nurse should don sterile gloves before cleaning the wound.
Option d is incorrect because the nurse should not cut a 4 x 4 piece of gauze to place around the drain site; instead, the nurse should use a pre-cut drain sponge.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
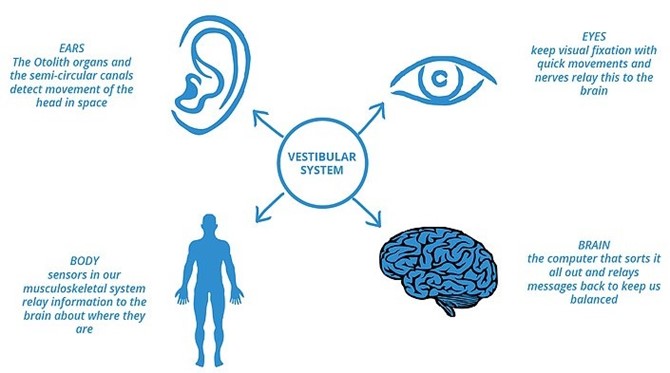
As individuals age, it is common for them to experience a decreased sense of balance. This can be attributed to age-related changes in the musculoskeletal system, sensory perception, and coordination. The inner ear, which plays a vital role in maintaining balance, undergoes natural degenerative changes over time. Additionally, age-related decline in muscle strength and flexibility can contribute to difficulties in maintaining balance. Therefore, a nurse assessing an older adult client should expect a decreased sense of balance as a common finding.
- Nighttime urinary incontinence: While nighttime urinary incontinence can occur in some older adults, it is not a universal finding. It is important to avoid making assumptions or generalizations about older adults experiencing urinary incontinence. Each individual's urinary function can vary, and incontinence can be influenced by various factors such as overall health, bladder capacity, medication use, and underlying medical conditions.
- Heightened sense of pain: Older adults may experience changes in pain perception due to age-related physiological changes and medical conditions. However, it is not a predictable or expected finding for all older adult clients. Pain perception can vary among individuals based on their overall health, chronic conditions, and individual pain thresholds. Therefore, while some older adults may experience heightened pain sensitivity, it is not a universal expectation.
- Increased nighttime sleeping: Sleep patterns can change with age, and older adults may experience alterations in their sleep-wake cycles. However, increased nighttime sleeping is not a definitive finding that applies to all older adult clients. Sleep patterns can vary greatly among individuals, and some older adults may experience decreased sleep duration or disrupted sleep rather than increased nighttime sleeping.
In summary, the nurse should expect a decreased sense of balance as a common finding when assessing an older adult client. It is important to approach each individual as unique and recognize that other findings such as nighttime urinary incontinence, heightened sense of pain, or increased nighttime sleeping may or may not be present, as they can vary among older adults based on individual factors.
Correct Answer is A
Explanation
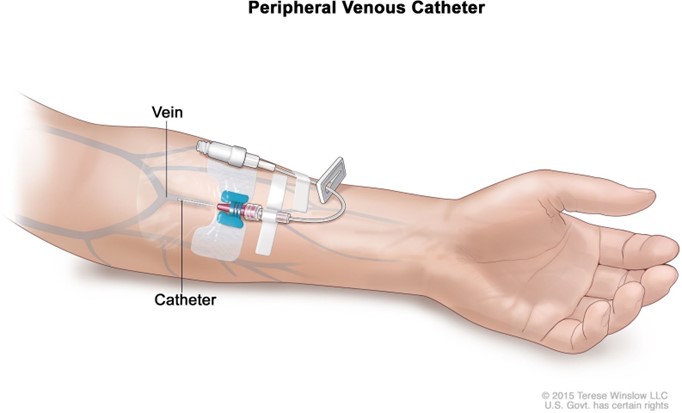
The correct answer is that the nurse should dangle the client's arm over the edge of the bed to help dilate the vein. This technique uses gravity to increase blood flow to the arm and dilate the veins, making it easier to insert a peripheral IV catheter.
Options b, c and d are not effective techniques for dilating a vein for IV insertion. Stroking the skin near the vein in an upward direction, instructing the client to flex their arm with the hand open and applying a cool compress to the vein for 10 min are not effective methods for dilating a vein.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today