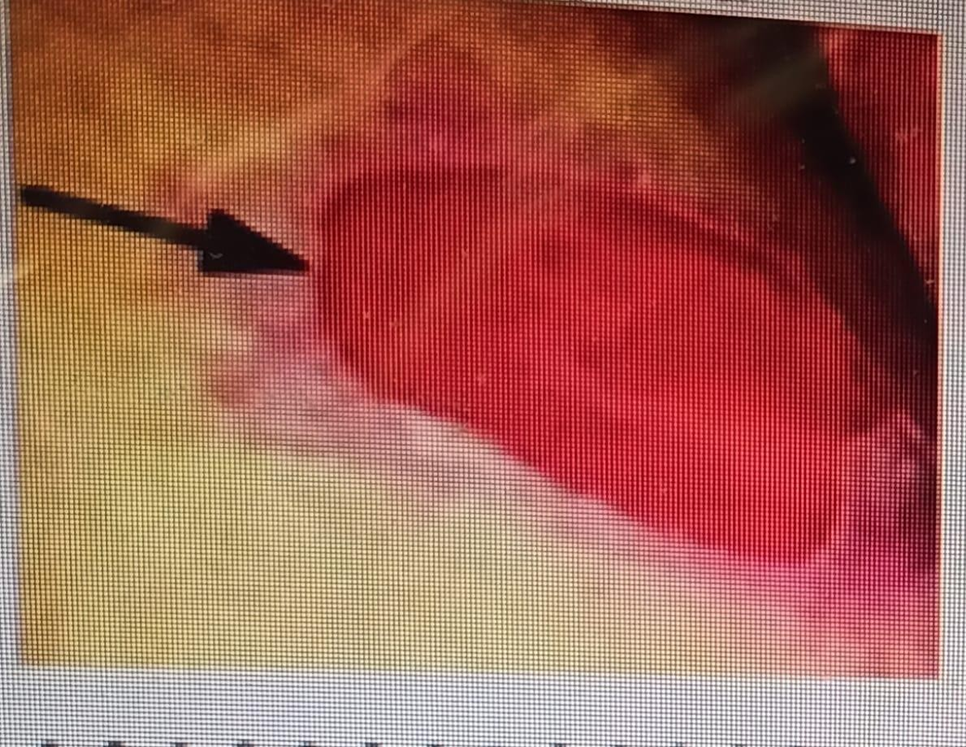
A nurse is completing her physical assessment on her newly admitted patient. She is assessing the patient's skin and documenting her findings. How should she document the following wound?

Stage I Pressure Ulcer
Stage II Pressure Ulcer
Stage IV Pressure Ulcer
Stage III Pressure Ulcer
The Correct Answer is B
Choice A rationale: Stage I pressure ulcers consist of non-blanching erythema with an intact epidermis unlike in the above picture.
Choice B rationale: This is correct since Stage II pressure ulcers involve partial-thickness skin loss but do not extend into the deeper layers as shown in the image above.
Choice C rationale: Stage IV pressure ulcers involve full-thickness tissue loss with exposed muscle, bone, or other structures.
Choice D rationale: Stage III pressure ulcers involve full-thickness tissue loss with visible fat but do not extend to the underlying muscle.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale: A client who is confined to bedrest may not need a gait belt as they are not ambulating.
Choice B rationale: A client with leg strength who can cooperate with movement is a likely candidate for a gait belt. This device provides support and stability during ambulation.
Choice C rationale: A client with a thoracic incision may not necessarily need a gait belt for ambulation unless there are specific mobility concerns.
Choice D rationale: A client with an abdominal incision may not necessarily need a gait belt for ambulation unless there are specific mobility concerns.

Correct Answer is D
Explanation
Choice A rationale: Lung sounds and chest x-ray are not directly relevant to assessing suspected food poisoning.
Choice B rationale: Routine urinalysis is not directly relevant to assessing suspected food poisoning.
Choice C rationale: Lung sounds and sputum sample are not directly relevant to assessing suspected food poisoning.
Choice D rationale: Bowel sounds and stool sample are relevant to assessing gastrointestinal symptoms associated with food poisoning.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today