A nurse is performing a skin assessment on a client who has a dark skin. Which one of the following locations on the client’s body should the nurse observe to access for jaundice?
Face
Shoulders
Palm of the hands
Sclera
The Correct Answer is D
Choice A reason:
Face is incorrect: Facial skin colour can vary for many reasons, but it may not be the best indicator of jaundice in individuals with dark skin.
Choice B reason
Shoulders is incorrect: The shoulders are not typically indicative of jaundice.
Choice C reason:
Palm of the hands is incorrect: While the palm of the hands can sometimes show yellowing in cases of jaundice, it is less reliable than observing the sclera.
Choice D reason:
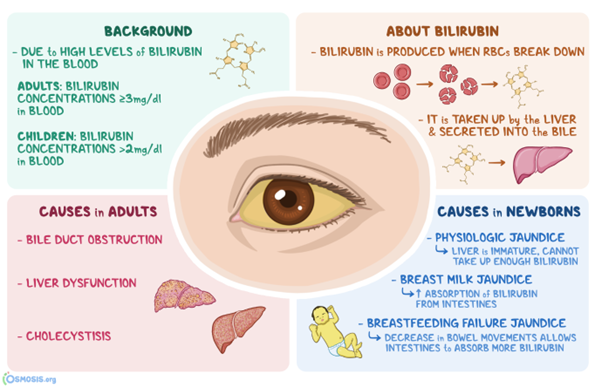
Sclera is the best location. In individuals with darker skin tones, yellowish discoloration of the skin due to jaundice can be more challenging to detect. However, the sclera of the eyes can still show noticeable yellowing, making it a reliable location for assessing jaundice in individuals with both light and dark skin.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
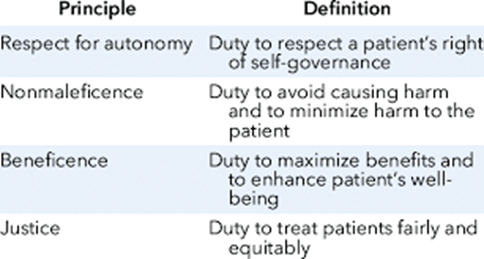
A. Autonomy is the ethical principle that respects the right of clients to make their own decisions and choices regarding their health care. Informed consent is a process that ensures that clients are fully informed of the benefits, risks, alternatives, and consequences of a proposed treatment or procedure, and that they voluntarily agree to it.
B. Nonmaleficence is the ethical principle that obliges health care providers to do no harm to clients, either intentionally or unintentionally. Informed consent does not directly promote this principle, although it may help to prevent harm by disclosing potential risks and complications.
C. Justice is the ethical principle that requires fair and equal treatment of all clients, regardless of their personal characteristics, preferences, or values. Informed consent does not directly promote this principle, although it may help to ensure that clients are not coerced or manipulated into accepting a treatment or procedure that they do not want or need.
D. Fidelity is the ethical principle that requires health care providers to be faithful and loyal to their clients, and to honor their commitments and promises. Informed consent does not directly promote this principle, although it may help to establish trust and rapport between clients and providers.
Correct Answer is B
Explanation
Choice A reason:
Natural loss of deciduous teeth is incorrect. Natural loss of deciduous teeth, also known as baby teeth, usually begins around the age of 5 or 6 years. At the age of 2, a toddler would still have their baby teeth.
Choice B reason:
This is a normal finding in toddlers. It is common for toddlers to have a protruding abdomen due to their body composition and the normal development of their abdominal muscles.
Choice C reason:
Head circumference exceeds chest circumference: In a typical 2-year-old toddler, the head circumference should be less than the chest circumference. The head grows rapidly during infancy and slows down as the child grows older, leading to a cage in the head-to-chest ratio.
Choice D reason:
The fontanels, or soft spots on the skull, usually close by the end of the first year. By age 2, the fontanels should be closed or very close to being closed, and they would not typically be palpable.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today