A nurse is performing an assessment on a postpartum patient.
The uterus is found to be displaced to the right.
Which of the following actions should the nurse take?
Action A.
Action B.
Action C.
Action D.
The Correct Answer is B
Choice A rationale:
Placing the mother in Trendelenburg's position would not correct the uterine displacement. Trendelenburg's position involves
lowering the head of the bed and raising the feet, which can actually worsen uterine displacement by increasing pressure on
the uterus from the abdominal organs.
It is not indicated for uterine displacement and could potentially have adverse effects on the patient's hemodynamic status
and respiratory function.
Choice C rationale:
Notifying the physician is important, but it is not the first action the nurse should take.
The nurse should assess the patient and attempt to correct the displacement before notifying the physician.
Choice D rationale:
Recording the findings is important for documentation, but it is not an intervention that will correct the uterine displacement.
Choice B rationale:
Massaging the fundus is the correct action to take when a postpartum uterus is displaced.
The fundus is the top of the uterus, and massaging it can help to stimulate the uterine muscles to contract and return to their
normal position.
This is often effective in correcting mild to moderate uterine displacements.
Here are the steps involved in massaging the fundus:
Locate the fundus: The nurse should first locate the fundus by palpating the abdomen just below the umbilicus.
Apply gentle pressure: Once the fundus is located, the nurse should apply gentle pressure with the fingertips in a circular
motion.
Continue massaging: The massage should be continued for several minutes, or until the uterus is felt to be firm and in the
midline position.
Additional notes:
If the uterine displacement is severe, or if the patient is experiencing pain or bleeding, the nurse should notify the physician
immediately.
Other interventions that may be used to correct uterine displacement include:
Assisting the patient to empty her bladder
Straight catheterization
Administration of oxytocin to stimulate uterine contractions
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A rationale:
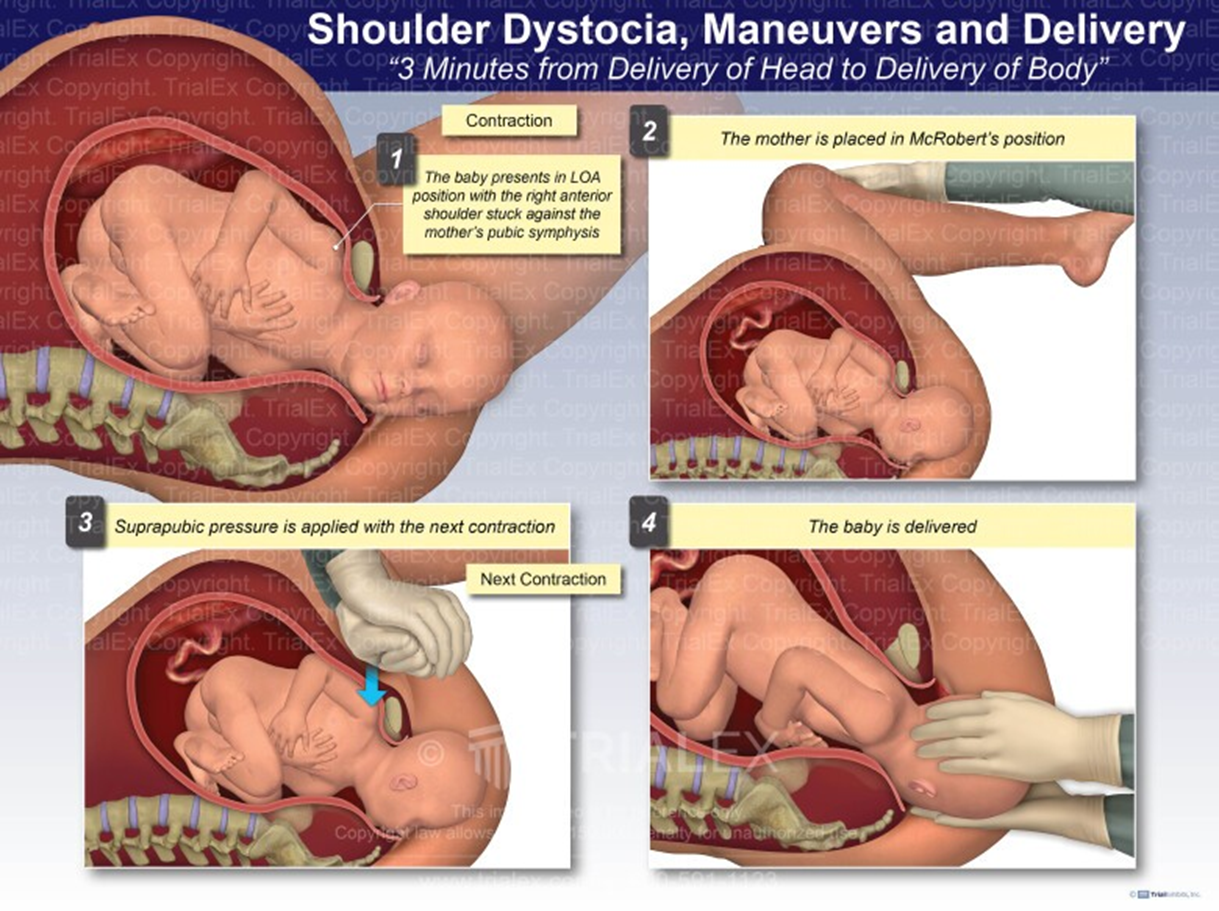
Normal progression of labor: After the fetal head is delivered, the shoulders typically follow immediately. The nurse should be prepared to assist with the delivery of the shoulders to ensure a safe and smooth birth process.
Significance of retraction: Retraction of the fetal head against the maternal perineum, also known as the "turtle sign," is a classic indicator of shoulder dystocia. While this sign does not guarantee shoulder dystocia, it warrants immediate preparation for potential management.
Anticipating shoulder dystocia: By anticipating the possibility of shoulder dystocia, the nurse can take proactive measures to minimize risks and facilitate delivery. These measures may include:
Positioning the mother appropriately (e.g., McRoberts maneuver)
- Applying suprapubic pressure
- Performing internal maneuvers (e.g., Rubin's maneuver)
- Breaking the clavicle (in extreme cases)
Choice B rationale:
Ineffective in shoulder dystocia: Encouraging the mother to push during the next contraction is not an effective intervention
for shoulder dystocia. In fact, excessive pushing can worsen the impaction of the shoulders and potentially lead to
complications such as fetal hypoxia, brachial plexus injury, or maternal perineal trauma.
Choice C rationale:
Necessary in confirmed dystocia: Calling for additional medical support is crucial if shoulder dystocia is confirmed. However,
immediate preparation for shoulder delivery should commence without delay, as prompt action is essential to prevent adverse
outcomes.
Choice D rationale:
Secondary concern: While pain relief medication may be administered for maternal comfort, it is not a priority intervention in
this situation. The primary focus should be on managing the potential shoulder dystocia and ensuring the safe delivery of the
baby.
Correct Answer is C
Explanation
Choice C rationale:
Endometritis is an inflammation of the inner lining of the uterus (endometrium). It is a common complication after childbirth,
affecting up to 1 in 10 women who deliver vaginally. Symptoms of endometritis typically develop within 1-3 days after
childbirth, but they can sometimes take up to a week to appear.
Swelling in the ankles is a common symptom of endometritis. This is because endometritis can cause inflammation and fluid
buildup in the pelvis, which can put pressure on the veins in the legs and cause them to swell.
Choice A rationale:
An increased heart rate can be a symptom of endometritis, but it is not a specific symptom. An increased heart rate can also be
caused by many other factors, such as fever, dehydration, and anxiety.
Choice B rationale:
Decreased appetite can be a symptom of endometritis, but it is not a specific symptom. Decreased appetite can also be caused
by many other factors, such as pain, fatigue, and nausea.
Choice D rationale:
Dry skin is not a typical symptom of endometritis. Dry skin can be caused by many other factors, such as dehydration,
medications, and underlying medical conditions.
Therefore, the most likely manifestation of endometritis in this patient is swelling in the ankles.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today