A nurse is assisting with the care of a client who is in labor.
The client's labor is difficult and prolonged and she reports a severe backache.
Which of the following factors is a contributing cause of difficult, prolonged labor?
Fetal attitude is in general flexion
Fetal lie is longitudinal
Maternal pelvis is gynecoid
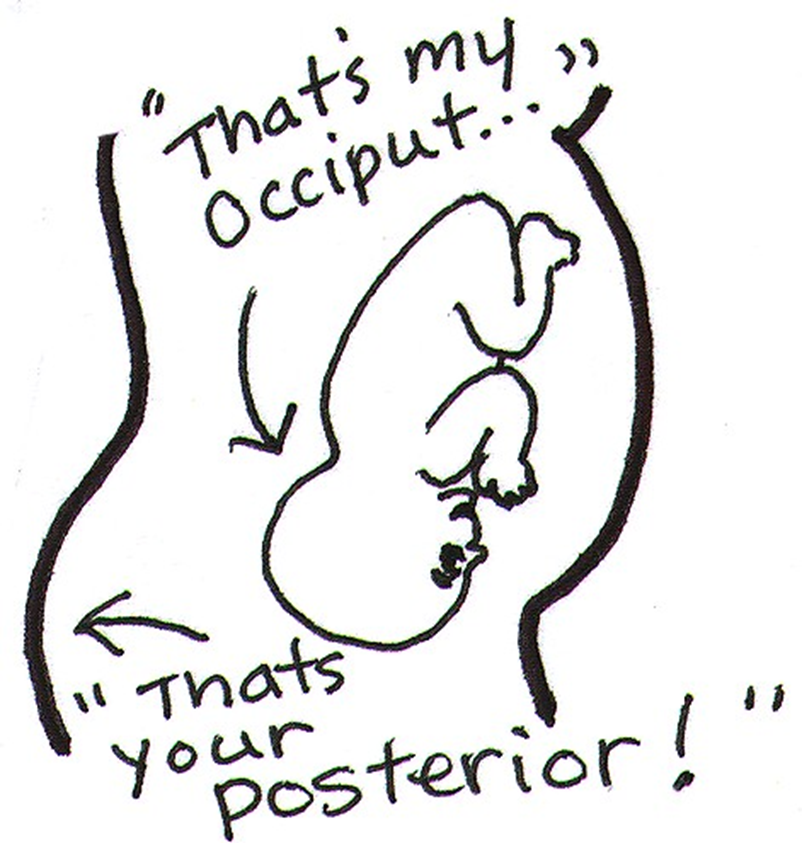
Fetal position is persistent occiput posterior
The Correct Answer is D
Choice A rationale:
Fetal attitude in general flexion is not a contributing factor to difficult, prolonged labor. In fact, it is the normal fetal attitude
during labor. The fetus is typically in a position of general flexion, where the head is flexed forward, chin to chest, and the arms
and legs are flexed, with the arms crossed over the chest and the legs bent at the knees.
Choice B rationale:
Fetal lie being longitudinal is the normal and most common fetal lie during labor. In a longitudinal lie, the long axis of the fetus
is parallel with the long axis of the mother. This is the ideal and most common position for labor and delivery.
Choice C rationale:
A gynecoid pelvis is the most common type of female pelvis and is the most favorable for childbirth. It has a round shape with
a wide pubic arch, which allows for easier passage of the baby during delivery.
Choice D rationale:
A persistent occiput posterior (OP) position can indeed contribute to difficult, prolonged labor. In an OP position, the baby’s
occipital bone is towards the mother’s posterior side. This position can cause labor to be more painful and last longer because the baby’s head diameter that presents to the birth canal is larger. It can also cause back pain during labor, often referred to as "back labor"1.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A rationale:
There is no evidence to suggest that epidural anesthesia delays the rupture of fetal membranes. The timing of rupture of fetal
membranes is influenced by various factors, including the strength of uterine contractions, the position of the baby, and the
elasticity of the amniotic sac. Epidural anesthesia does not directly affect these factors.
Choice B rationale:
Epidural anesthesia can prolong labor by interfering with the natural process of labor. It can weaken uterine contractions,
slow down cervical dilation, and potentially lead to a prolonged second stage of labor. This is because the anesthesia blocks the
nerve signals that control the muscles of the uterus. When these signals are blocked, the contractions may become less
frequent and less intense. This can delay the progress of labor and increase the risk of interventions such as forceps delivery
or cesarean section.
Choice C rationale:
While epidural anesthesia can have some effects on the baby, it is not a primary cause of fetal depression. Fetal depression is
typically caused by other factors, such as decreased oxygen supply to the baby, maternal infection, or placental problems.
Epidural anesthesia can sometimes lead to a temporary decrease in the baby's heart rate, but this is usually well-managed by
the healthcare team and does not typically lead to significant fetal depression.
Choice D rationale:
Epidural anesthesia does not typically cause maternal hypertension. In fact, it can sometimes have the opposite effect and
cause a slight decrease in blood pressure. This is because the anesthesia can relax the blood vessels, which can lead to a drop
in blood pressure. However, this is usually not a significant concern and is easily managed by the healthcare team.
Correct Answer is D
Explanation
Choice A rationale:
Rh positive individuals already have the Rh factor on their red blood cells, so they do not need Rho(D) immune globulin to
prevent sensitization.
The newborn being Rh positive does not pose a risk to an Rh positive mother, as their blood types are compatible.
Choice B rationale:
Rh positive individuals cannot develop antibodies against the Rh factor, as it is already present on their own red blood cells.
The newborn's Rh negative status does not create a risk of sensitization for the mother, as there is no Rh factor to trigger an
immune response.
Choice C rationale:
If both the mother and the newborn are Rh negative, there is no risk of Rh incompatibility.
This is because neither individual has the Rh factor on their red blood cells, so there is no potential for sensitization.
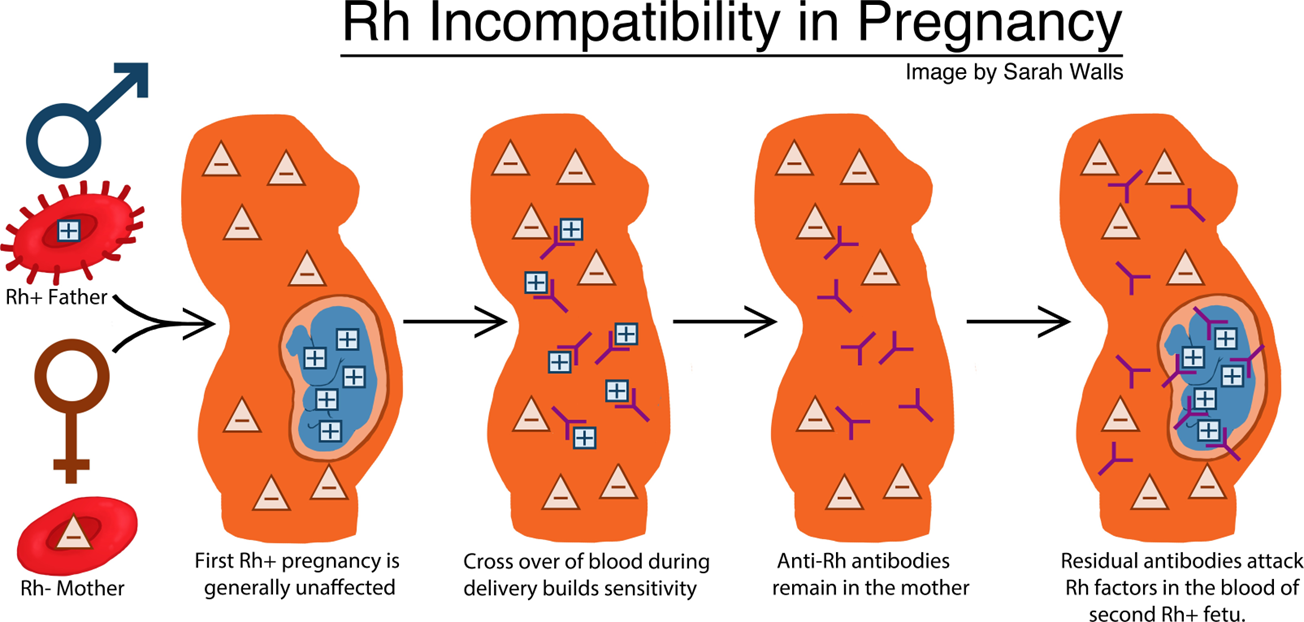
Choice D rationale:
When an Rh negative mother carries an Rh positive fetus, there is a risk of Rh sensitization during pregnancy and delivery.
This occurs when fetal blood cells cross the placenta and enter the mother's bloodstream, exposing her immune system to the
Rh factor.
If the mother's immune system recognizes the Rh factor as foreign, it can produce antibodies against it.
These antibodies can cross the placenta in subsequent pregnancies and attack the red blood cells of Rh positive fetuses,
leading to hemolytic disease of the newborn (HDN).
Rho(D) immune globulin is a medication that can prevent Rh sensitization by binding to Rh positive fetal blood cells that have
entered the mother's bloodstream.
This prevents the mother's immune system from recognizing the Rh factor and producing antibodies.
Rho(D) immune globulin is typically given to Rh negative mothers within 72 hours of delivery of an Rh positive newborn, as well as after other events that could lead to Rh sensitization, such as miscarriage, abortion, or ectopic pregnancy.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today