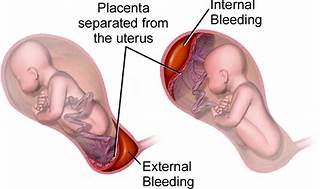
A nurse is reinforcing teaching with a client who is at 34 weeks of gestation and at risk for placental abruption. Does the nurse recognize that which of the following is the most common risk factor for a placental abruption?
Maternal hypertension.
Maternal cocaine use.
Maternal cigarette smoking.
Maternal battering.
The Correct Answer is A
The correct answer is choice A, Maternal hypertension.
Choice A rationale:
Maternal hypertension is widely recognized as the most common risk factor for placental abruption. High blood pressure can cause the placenta to detach from the uterine wall, leading to abruption. In summary, while all the listed factors can contribute to the risk of placental abruption, maternal hypertension stands out as the most common cause, supported by multiple health sources. It’s important for nurses to recognize and manage hypertension in pregnant clients to minimize the risk of this serious complication.
Choice B rationale:
While maternal cocaine use is a significant risk factor for placental abruption due to its vasoconstrictive effects, which can compromise the placental blood flow, it is not as common as maternal hypertension.
Choice C rationale:
Maternal cigarette smoking is also a risk factor for placental abruption. Smoking can lead to a variety of complications in pregnancy, including placental problems, but again, it is less common than hypertension as a cause for abruption.
Choice D rationale:
Maternal battering can lead to trauma which may result in placental abruption. However, it is not considered the most common risk factor when compared to maternal hypertension.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A rationale:
The umbilical cord typically contains two arteries and one vein. Arteries carry oxygen-depleted blood and waste products from the fetus to the placenta for removal, while the vein carries oxygenated blood and nutrients from the placenta to the fetus. This arrangement is essential for maintaining proper fetal circulation during pregnancy.
Choice B rationale:
This choice is incorrect because the umbilical cord usually contains two arteries and one vein, not just one artery and one vein. Having only one artery could indicate a potential vascular abnormality or congenital issue that may require further investigation or medical attention.
Choice C rationale:
This is the correct answer. The umbilical cord usually contains two arteries and one vein. The presence of two arteries allows for the efficient removal of waste products and carbon dioxide from the fetus, while the single vein delivers essential nutrients and oxygen to support the baby's growth and development.
Choice D rationale:
This choice is incorrect as it states two veins and one artery, which is not the typical configuration of blood vessels in the umbilical cord. Having two veins and one artery would disrupt fetal circulation and hinder proper nutrient and waste exchange between the fetus and the placenta.
Correct Answer is D
Explanation
Choice A rationale:
Helping the client to the bathroom to empty her bladder is not the appropriate response in this situation. The client's sudden urge to push indicates that she is in the second stage of labour, which is the pushing phase. The cervix is already dilated at 7 cm, and the fetus is at 1+ station, indicating that delivery is imminent. Emptying the bladder at this point is not a priority and may delay necessary actions.
Choice B rationale:
Assisting the client into a comfortable position is also not the appropriate response. The client's urge to push suggests that she is in the active stage of labor, and her cervix is already 7 cm dilated. Encouraging a comfortable position might not be suitable since the focus should be on monitoring the progress of labor and preparing for delivery.
Choice C rationale:
Having the client pant during the next few contractions is not the correct response either. Panting is typically recommended during the transition phase of labor to prevent rapid pushing and potential damage to the perineum. However, in this scenario, the client is already fully dilated, and the fetus is at 1+ station, indicating that the second stage of labour has commenced. Panting is not necessary at this point.
Choice D rationale:
The appropriate nursing response is to assess the perineum for signs of crowning. The sudden urge to push indicates that the baby is descending through the birth canal and may be close to crowning, which is when the baby's head becomes visible at the vaginal opening. By assessing for crowning, the nurse can determine if delivery is imminent and notify the healthcare provider for further actions and preparation for the baby's birth.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today