A nurse is reviewing the plan of care for a group of clients. The nurse should identify that informed consent is required for which of the following procedures?
Irrigation of a wound with antibiotic solution
Administration of an iron injection using Z-track technique
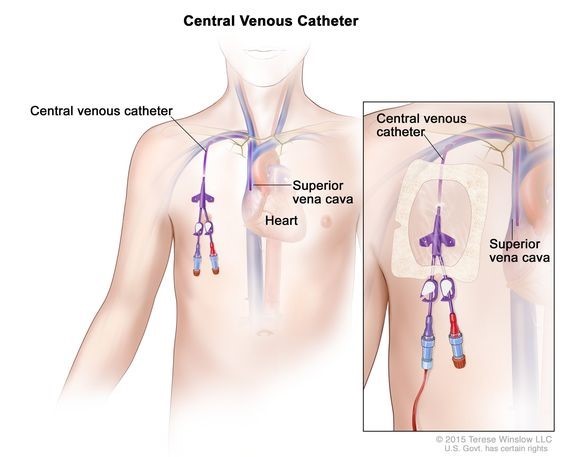
Placement of a central venous catheter
Insertion of a nasogastric tube
The Correct Answer is C
Informed consent is a legal and ethical requirement for certain medical procedures. It involves providing the client with clear and comprehensive information about the procedure, including its risks, benefits, alternatives, and expected outcomes. The client must understand the information provided and voluntarily give their consent before the procedure can be performed.
Placement of a central venous catheter is an invasive procedure that carries risks and potential complications, making it necessary to obtain informed consent from the client.
Wound irrigation with an antibiotic solution is a standard nursing intervention for wound care and does not usually involve invasive procedures. Informed consent is not typically required for this procedure.
The administration of an iron injection using the Z-track technique is a standard nursing procedure. While it involves an injection, it is not typically considered an invasive procedure that would require informed consent.
Insertion of a nasogastric tube is a common procedure that involves passing a tube through the nose and into the stomach for various purposes, such as feeding, decompression, or medication administration. While it is an invasive procedure, it is often performed in emergency or critical care situations where the client's immediate well-being takes precedence. Informed consent may not be feasible or necessary in these situations, depending on the context and urgency.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Explanation
C. Skin rash with fever
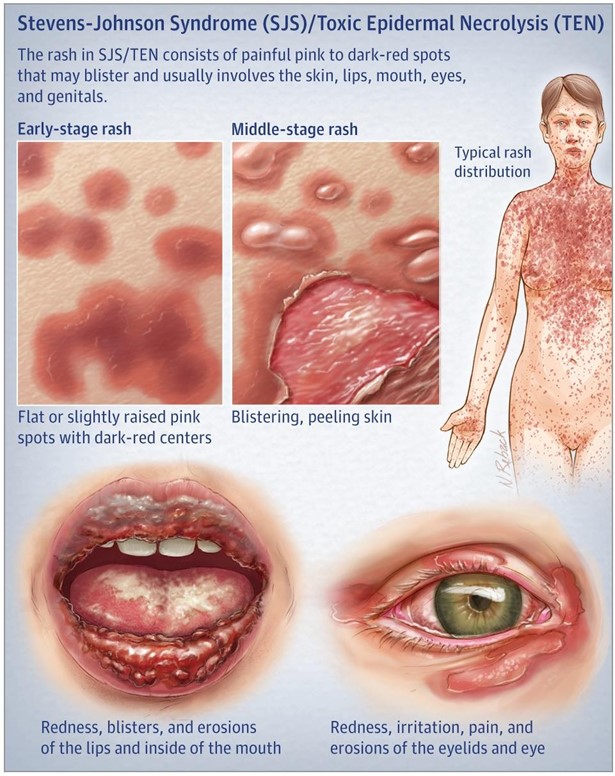
Stevens-Johnson syndrome (SJS) is a severe and potentially life-threatening hypersensitivity reaction that can occur as a rare side effect of certain medications, including allopurinol.
Monitoring and early recognition of SJS symptoms are crucial for prompt medical.
Skin rash with fever is a hallmark manifestation of Stevens-Johnson syndrome. It often starts with flu-like symptoms such as fever and malaise, followed by the appearance of a widespread, painful, and rapidly progressing rash. The rash typically involves the mucous membranes, including the mouth, nose, and eyes, and can be accompanied by blisters or sores. Prompt reporting of these symptoms is critical for early diagnosis and intervention.
Tinnitus with ear pain in (option A) is incorrect because it is not typically associated with Stevens- Johnson syndrome. It may indicate another condition or side effect unrelated to SJS.
Hyperreflexia, which refers to abnormally increased reflexes, in (option B) is incorrect because it is not a characteristic manifestation of Stevens-Johnson syndrome. It may indicate a neurological condition or reaction to another medication, but it is not specific to SJS.
Diplopia, or double vision, in option (D) is incorrect because it is not commonly associated with Stevens- Johnson syndrome. It may be caused by other ocular or neurological conditions.
In summary, the nurse should instruct the client taking allopurinol to monitor and report the manifestation of a skin rash with fever. This is important because it may indicate the development of Stevens-Johnson syndrome, a severe and potentially life-threatening reaction to the medication. Early recognition and medical intervention are crucial to minimize complications and ensure appropriate treatment.
Correct Answer is C
Explanation
Nausea and vomiting are common side effects of doxycycline, an antibiotic commonly used to treat chlamydial infections. Taking the medication with food or a snack can help alleviate these side effects. The recommendation to take the medication with crackers provides a light source of carbohydrates that can help settle the stomach and reduce nausea.
It is generally not recommended to take doxycycline with calcium-rich foods or beverages, as they can interfere with the absorption of the medication. Calcium can form complexes with doxycycline, reducing its effectiveness. Therefore, it is best to avoid calcium-rich foods and beverages, including calcium-fortified orange juice, when taking doxycycline.
Similar to calcium-rich foods, antacids can also interfere with the absorption of doxycycline. Antacids contain aluminum, magnesium, or calcium, which can bind to doxycycline and reduce its effectiveness. Therefore, it is generally recommended to avoid taking doxycycline with antacids.
While it is important to remain upright for a short period after taking some medications to prevent reflux or aspiration, this recommendation may not specifically address the client's nausea and vomiting. Taking the medication with food, such as crackers, may be more effective in alleviating the symptoms.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today