A nurse is teaching a client who has major depressive disorder about electroconvulsive therapy. Which of the following information should the nurse include?
"This therapy works as a cure for major depressive disorders."
"You will be awake and alert during the procedure."
"You might experience confusion for a few hours after treatment."
"This therapy will stimulate the vagus nerve to improve your mood."
The Correct Answer is C
Choice A reason:
Electroconvulsive therapy (ECT) is not considered a cure for major depressive disorders. While ECT can be highly effective in alleviating symptoms of severe depression, it does not prevent future episodes. Patients often require ongoing treatment with medications or psychotherapy to maintain the benefits of ECT.
Choice B reason:
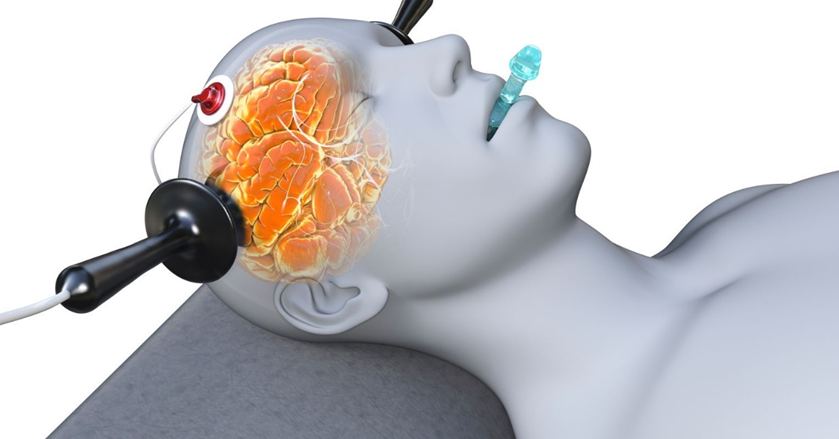
During ECT, the patient is not awake and alert. The procedure is performed under general anesthesia, meaning the patient is unconscious and does not feel the electrical stimulation or the induced seizure. This ensures the procedure is painless and the patient is unaware during the treatment.
Choice C reason:
It is common for patients to experience confusion for a few hours after ECT. This confusion is partly due to the anesthesia and partly due to the treatment itself. In most cases, the confusion resolves within a few hours, but it can sometimes last longer, especially in older adults.
Choice D reason:
ECT does not stimulate the vagus nerve. Vagus nerve stimulation (VNS) is a different treatment that involves using a device to send electrical impulses to the vagus nerve. ECT works by inducing a controlled seizure in the brain, which can help alleviate symptoms of severe depression.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason:
Cocaine is a powerful stimulant drug that can cause an acute increase in heart rate and blood pressure. Hypertension is a common clinical manifestation associated with cocaine use due to its sympathomimetic effects, which stimulate the sympathetic nervous system. This can lead to vasoconstriction and increased cardiac output, resulting in elevated blood pressure levels.
Choice B reason:
Hypothermia is not typically associated with cocaine use. Cocaine tends to increase body temperature due to its stimulant properties, which can lead to hyperthermia rather than hypothermia. If hypothermia is present in a client who has used cocaine, it may be due to other factors or substances that the client has ingested.
Choice C reason:
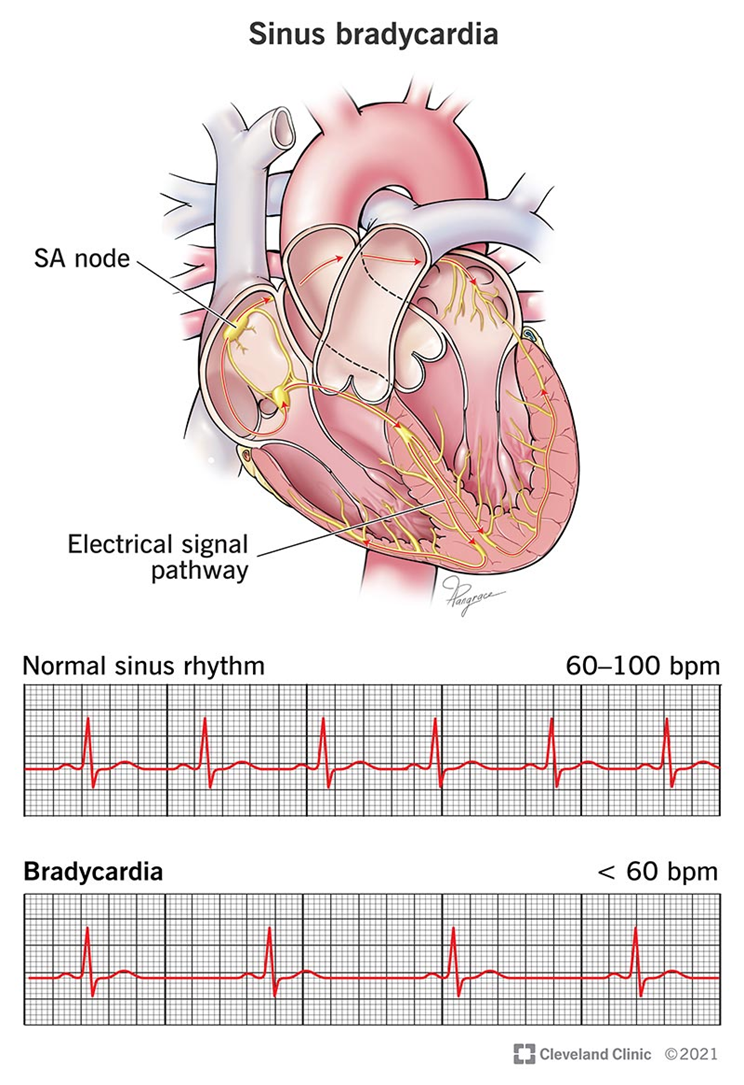
Bradycardia, or a slower than normal heart rate, is not a common effect of cocaine use. Cocaine usually causes tachycardia, an increased heart rate, as part of its stimulant effect on the body. Bradycardia would be an unusual response and might suggest other medical issues or the influence of other substances.
Correct Answer is B
Explanation
Choice A reason:
An apology from the client for their prior behavior, while it may be a positive step towards recovery, does not necessarily indicate that they have regained control over their actions or that they no longer pose a risk to themselves or others. The decision to discontinue restraints should be based on current behavior and risk assessment rather than past actions.
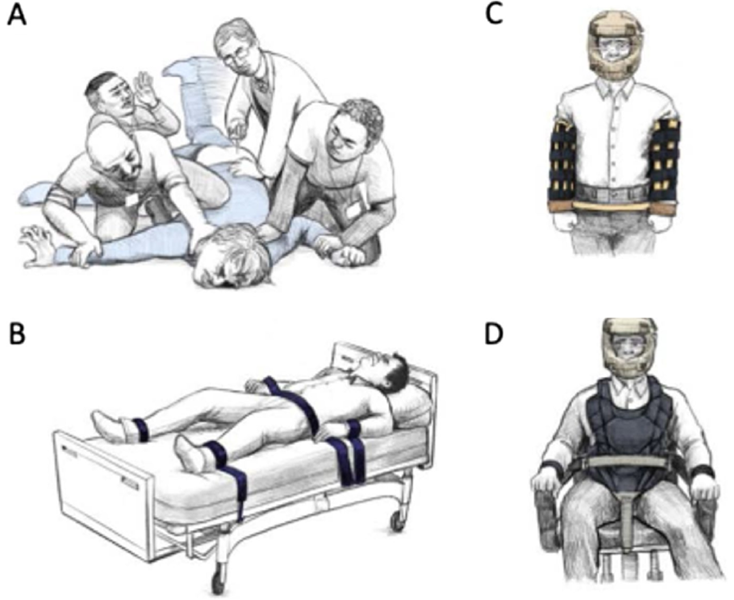
Choice B reason:
The primary goal of using physical restraints is to prevent harm to the patient or others when less restrictive interventions are not effective. If the client demonstrates control over their actions, it suggests that they are no longer at immediate risk of harm, and therefore, discontinuing restraints could be considered³⁴⁵. This aligns with guidelines that advocate for restraint use to be continually assessed and reduced or discontinued as soon as possible.
Choice C reason:
While a request to be released from restraints indicates a desire for freedom, it does not provide enough information about the client's current mental state or risk of harm. The healthcare team must assess whether the client's condition has improved to a point where restraints are no longer necessary.
Choice D reason:
Signing a behavioral contract is a positive step towards establishing trust and setting expectations for behavior. However, it is not an immediate indication that the client can safely have restraints removed. The effectiveness of such contracts depends on the individual's ability to understand and adhere to the agreed-upon behaviors.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today