A nurse is teaching a client who is on a low-sodium diet. Which of the following instructions should the nurse include? (Select all that apply.)
Limit intake of canned soups.
Choose botled salad dressings.
Choose diet sodas over botled water.
Replace processed meats with fresh meat products.
Read labels on foods before eating.
Correct Answer : A,D,E
Choice A: Limit intake of canned soups is correct because canned soups are high in sodium and can increase blood
pressure and fluid retention. The nurse should advise the client to choose low-sodium or homemade soups instead.
Choice B: Choose botled salad dressings is incorrect because botled salad dressings are also high in sodium and can have added sugars and fats. The nurse should advise the client to make their own salad dressings with vinegar, oil, herbs, and spices.
Choice C: Choose diet sodas over botled water is incorrect because diet sodas are not a healthy alternative to water. Diet sodas contain artificial sweeteners, caffeine, and phosphoric acid, which can affect the body's pH balance and calcium absorption. The nurse should advise the client to drink plain water or flavored water with natural ingredients.
Choice D: Replace processed meats with fresh meat products is correct because processed meats such as bacon, ham, sausage, and hot dogs are high in sodium and preservatives. The nurse should advise the client to choose fresh meat products such as chicken, turkey, fish, or lean beef.
Choice E: Read labels on foods before eating is correct because reading labels can help the client identify the sodium content and other ingredients in foods. The nurse should advise the client to look for foods that have less than 140 mg of sodium per serving and avoid foods that have salt, sodium, or monosodium glutamate (MSG) in the ingredient list.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A Reason: This is correct because 600 milliliters is a low volume of urine output for a 24-hour period, which indicates oliguria. Oliguria is defined as urine output less than 400 to 500 milliliters per day or less than 30 milliliters per hour. Oliguria can be a sign of dehydration, kidney injury, urinary obstruction, or shock. The nurse should notify the patient's healthcare provider and monitor the patient's fluid balance, vital signs, and laboratory values.
Choice B Reason: This is incorrect because 1200 milliliters is a normal volume of urine output for a 24-hour period, which indicates adequate renal function. The normal range of urine output for adults is 800 to 2000 milliliters per day or 30 to 80 milliliters per hour. The nurse should document the patient's urine output and continue to assess the patient's recovery status.
Choice C Reason: This is incorrect because 1800 milliliters is a normal volume of urine output for a 24-hour period, which indicates adequate renal function. The normal range of urine output for adults is 800 to 2000 milliliters per day or 30 to 80 milliliters per hour. The nurse should document the patient's urine output and continue to assess the patient's recovery status.
Choice D Reason: This is incorrect because 750 milliliters is a low-normal volume of urine output for a 24-hour period, which does not require immediate intervention. However, the nurse should be alert for any signs of decreased renal perfusion or function, such as hypotension, tachycardia, decreased urine specific gravity, or elevated blood urea nitrogen (BUN) and creatinine levels. The nurse should encourage the patient to drink fluids as tolerated and report any changes in urine output or quality.
Choice E Reason: This is incorrect because 1000 milliliters is a normal volume of urine output for a 24-hour period, which indicates adequate renal function. The normal range of urine output for adults is 800 to 2000 milliliters per day or 30 to 80 milliliters per hour. The nurse should document the patient's urine output and continue to assess the patient's recovery status.
Correct Answer is C
Explanation
Choice A: Corticosteroid is incorrect because it does not directly affect the potassium level in the blood, although it can cause sodium and water retention, which can dilute the potassium concentration. Corticosteroid is a type of anti- inflammatory medication that can be used to treat conditions such as asthma, arthritis, or allergic reactions.
Choice B: Narcotic is incorrect because it does not directly affect the potassium level in the blood, although it can cause respiratory depression, which can lead to respiratory acidosis and hyperkalemia, or high potassium level. Narcotic is a type of analgesic medication that can be used to treat moderate to severe pain.
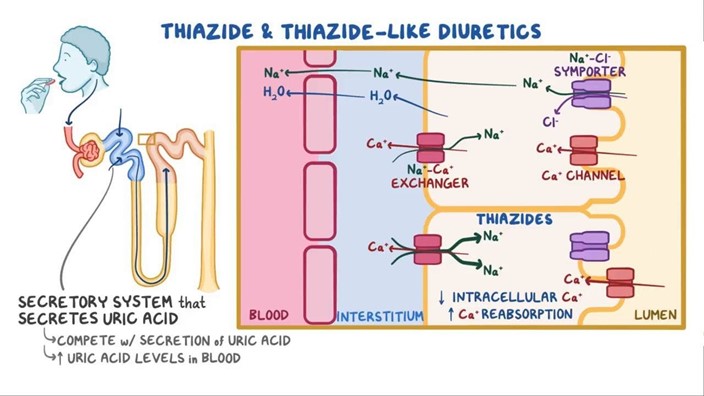
Choice C: Thiazide diuretic is correct because it is a type of medication that increases urine output and sodium excretion, but also causes potassium loss in the urine. Thiazide diuretic can be used to treat conditions such as hypertension, edema, or heart failure.
Choice D: Muscle relaxer is incorrect because it does not directly affect the potassium level in the blood, although it can cause muscle weakness, which can mimic the symptoms of hypokalemia. Muscle relaxer is a type of medication that can be used to treat conditions such as muscle spasms, back pain, or fibromyalgia.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today