After initiating a steroid nebulizer treatment for a client with asthma in respiratory distress, which intervention is most important for the nurse to implement?
Monitor pulse oximetry every 2 hours.
Teach proper use of a rescue inhaler.
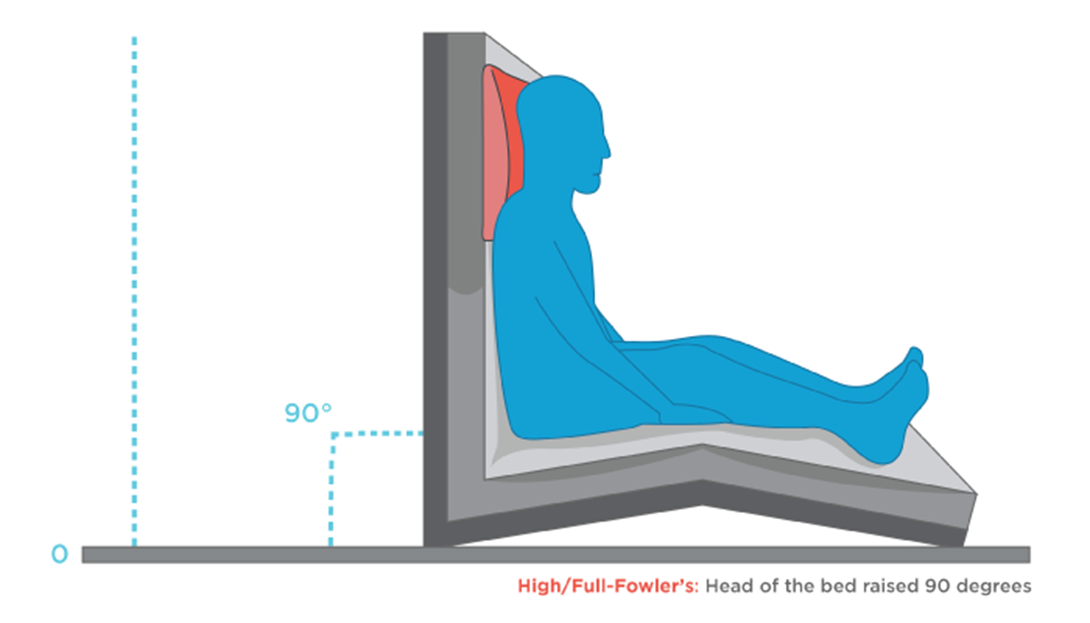
Elevate the head of bed to 90 degrees.
Determine exposure to asthmatic triggers.
The Correct Answer is C
Choice A reason: This is incorrect because monitoring pulse oximetry every 2 hours is not a sufficient or timely intervention for the nurse to implement. Pulse oximetry is a noninvasive method of measuring the oxygen saturation of hemoglobin in the blood. Normal oxygen saturation is 95% to 100%, while hypoxemia is less than 90%. However, pulse oximetry may not reflect the severity of respiratory distress or the effectiveness of nebulizer treatment in a client with asthma. Moreover, monitoring pulse oximetry every 2 hours is too infrequent for a client who is in acute respiratory distress and needs more frequent assessment and intervention.
Choice B reason: This is incorrect because teaching proper use of a rescue inhaler is not a priority or relevant intervention for the nurse to implement. A rescue inhaler is a type of short-acting bronchodilator that can be used to relieve acute asthma symptoms by relaxing the smooth muscles of the airways and improving airflow. However, teaching proper use of a rescue inhaler is not an urgent action for a client who is already receiving nebulizer treatment, which delivers a higher dose of medication directly to the lungs. Moreover, teaching proper use of a rescue inhaler is not appropriate for a client who is in respiratory distress and may not be able to focus or retain information.
Choice C reason: This is correct because elevating the head of bed to 90 degrees is the most important intervention for the nurse to implement. Elevating the head of bed to 90 degrees can help improve breathing and oxygenation by reducing pressure on the diaphragm and chest wall, increasing lung expansion and ventilation, and facilitating expectoration of mucus. This can enhance the effects of nebulizer treatment and reduce respiratory distress in a client with asthma.
Choice D reason: This is incorrect because determining exposure to asthmatic triggers is not an immediate or helpful intervention for the nurse to implement. Asthmatic triggers are substances or factors that can cause or worsen asthma symptoms by inducing inflammation or constriction of the airways. Examples of asthmatic triggers include allergens, irritants, infections, exercise, stress, or weather changes. However, determining exposure to asthmatic triggers is not a priority action for a client who is in respiratory distress and needs more urgent interventions to improve breathing and oxygenation. Moreover, determining exposure to asthmatic triggers may not change the management or outcome of an acute asthma attack that has already occurred.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","D","E"]
Explanation
Choice A reason: This is correct because abdominal obesity, also known as central obesity or visceral fat, is one of the criteria for diagnosing metabolic syndrome and a major risk factor for diabetes mellitus and vascular disease. Abdominal obesity is defined as having a waist circumference of more than 40 inches (102 cm) for men or 35 inches (88 cm) for women. Abdominal obesity can increase insulin resistance, inflammation, and blood pressure, which can lead to impaired glucose metabolism and cardiovascular complications.
Choice B reason: This is correct because blood pressure of 150/96 mm Hg is another criterion for diagnosing metabolic syndrome and a significant risk factor for diabetes mellitus and vascular disease. Blood pressure is defined as the force exerted by blood against the walls of blood vessels. Normal blood pressure is less than 120/80 mm Hg, while high blood pressure (hypertension) is 140/90 mm Hg or higher. High blood pressure can damage the blood vessels and organs, such as the heart, kidneys, eyes, and brain, and increase the risk of heart attack, stroke, kidney failure, and vision loss.
Choice C reason: This is incorrect because elevated high density lipoproteins (HDL), also known as good cholesterol, are not a criterion for diagnosing metabolic syndrome or a risk factor for diabetes mellitus and vascular disease. In fact, HDL are beneficial for cardiovascular health because they help remove excess cholesterol from the blood and prevent plaque buildup in the arteries. Normal HDL levels are 40 mg/dL (1.0 mmol/L) or higher for men and 50 mg/dL (1.3 mmol/L) or higher for women.
Choice D reason: This is correct because increased triglyceride levels are another criterion for diagnosing metabolic syndrome and a risk factor for diabetes mellitus and vascular disease. Triglycerides are a type of fat that circulates in the blood and provides energy to cells. Normal triglyceride levels are less than 150 mg/dL (1.7 mmol/L), while high triglyceride levels are 200 mg/dL (2.3 mmol/L) or higher. High triglyceride levels can increase insulin resistance, inflammation, and blood clotting, which can impair glucose metabolism and increase the risk of heart attack and stroke.
Choice E reason: This is correct because hyperglycemia, also known as high blood sugar, is another criterion for diagnosing metabolic syndrome and a hallmark of diabetes mellitus. Hyperglycemia occurs when the body cannot produce enough insulin or use it properly to regulate the amount of glucose in the blood. Normal blood glucose levels are 70 to 99 mg/dL (3.9 to 5.5 mmol/L) before meals and less than 140 mg/dL (7.8 mmol/L) two hours after meals, while hyperglycemia is 126 mg/dL (7.0 mmol/L) or higher before meals or 200 mg/dL (11.1 mmol/L) or higher two hours after meals. Hyperglycemia can damage the blood vessels and organs, such as the eyes, kidneys, nerves, and feet, and increase the risk of infections, ulcers, amputations, and diabetic ketoacidosis.
Choice F reason: This is incorrect because hypothyroidism, also known as underactive thyroid, is not a criterion for diagnosing metabolic syndrome or a direct risk factor for diabetes mellitus and vascular disease. Hypothyroidism occurs when the thyroid gland does not produce enough thyroid hormones, which regulate the body's metabolism, growth, and development. Hypothyroidism can cause symptoms such as fatigue, weight gain, cold intolerance, dry skin, hair loss, constipation, and depression. However, hypothyroidism does not affect the blood glucose or lipid levels directly, but rather indirectly through its effects on weight and appetite.
Correct Answer is C
Explanation
Choice A: A headache rated at 0 on 0 to 10 scale is not a specific indicator of the effectiveness of an antihistamine. A headache may be caused by other factors, such as dehydration, stress, or sinus congestion.
Choice B: Oxygen saturation level of 99% is a normal finding and does not reflect the effect of an antihistamine. Oxygen saturation measures the amount of oxygen in the blood and can be affected by respiratory conditions, altitude, or smoking.
Choice C: Ambulating easily without vertigo is a sign that the antihistamine is effective. Vertigo is a common symptom of Ménière's disease, which is a disorder of the inner ear that causes episodes of spinning sensation, hearing loss, and tinnitus. Antihistamines can help reduce the fluid buildup in the inner ear and relieve vertigo.
Choice D: Blood pressure of 120/80 mm Hg is a normal finding and does not indicate the effect of an antihistamine. Blood pressure measures the force of blood against the walls of the arteries and can be influenced by factors such as heart rate, cardiac output, blood volume, and vascular resistance.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today