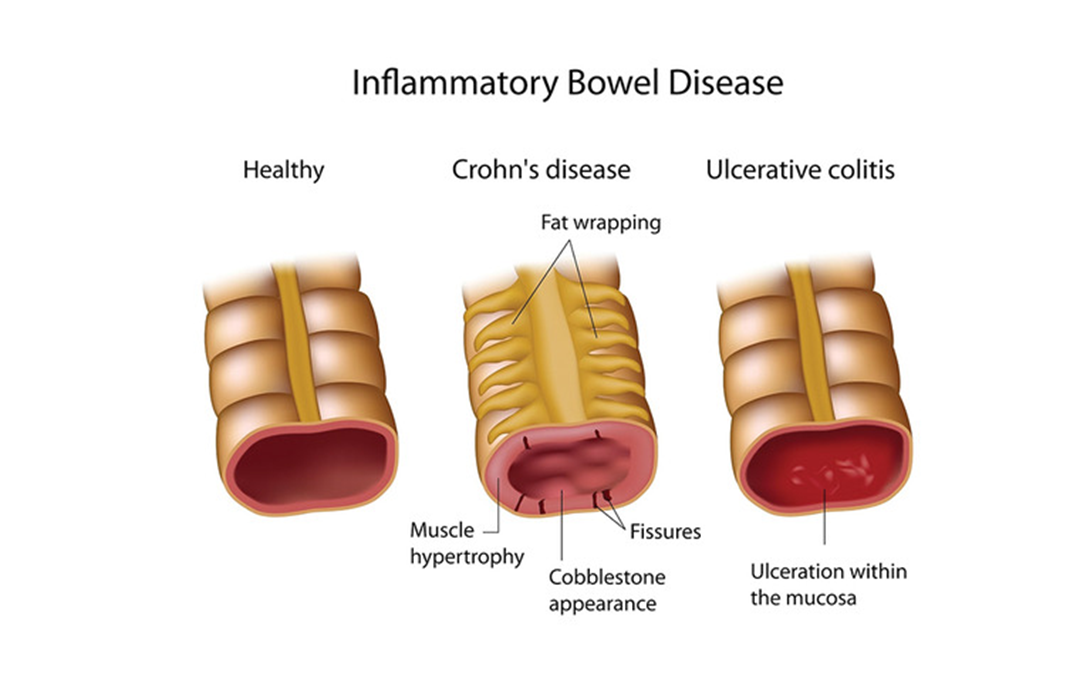
A client is hospitalized with an inflammatory bowel disease (IBD) exacerbation and is being treated with a corticosteroid. The client develops a rigid abdomen with rebound tenderness. Which action should the nurse take?
Measure capillary glucose level.
Encourage ambulation in the room.
Monitor for bloody diarrheal stools.
Obtain vital sign measurements.
The Correct Answer is D
Choice A reason: Measuring capillary glucose level is not a priority action for a client with a rigid abdomen and rebound tenderness. These signs indicate peritonitis, which is a serious complication of IBD that requires immediate attention. Corticosteroids can increase blood glucose levels, but this is not an urgent concern in this situation.
Choice B reason: Encouraging ambulation in the room is not appropriate for a client with a rigid abdomen and rebound tenderness. These signs indicate peritonitis, which is a serious complication of IBD that requires immediate attention. Ambulation can worsen the pain and inflammation, and increase the risk of bowel perforation.
Choice C reason: Monitoring for bloody diarrheal stools is important for a client with IBD, but not a priority action for a client with a rigid abdomen and rebound tenderness. These signs indicate peritonitis, which is a serious complication of IBD that requires immediate attention. Bloody stools can be a sign of ulceration or bleeding in the bowel, but they are not specific to peritonitis.
Choice D reason: Obtaining vital sign measurements is the priority action for a client with a rigid abdomen and rebound tenderness. These signs indicate peritonitis, which is a serious complication of IBD that requires immediate attention. Vital signs can reveal signs of infection, inflammation, shock, and organ failure, which can guide the appropriate interventions and treatments.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Sodium polystyrene sulfonate is a medication that binds to excess potassium in the gastrointestinal tract and removes it from the body through feces. It is used to treat hyperkalemia, which is a high level of potassium in the blood. Hyperkalemia can cause cardiac arrhythmias and muscle weakness, and it is a common complication of AKI. Therefore, this medication should be administered first to lower the potassium level and prevent life-threatening complications.
Choice B reason: Sevelamer is a medication that binds to phosphorus in the gastrointestinal tract and removes it from the body through feces. It is used to treat hyperphosphatemia, which is a high level of phosphorus in the blood. Hyperphosphatemia can cause bone loss and soft tissue calcification, and it is a common complication of chronic kidney disease (CKD). However, it is not an urgent issue in AKI, and it does not affect the potassium level.
Choice C reason: Calcium acetate is a medication that also binds to phosphorus in the gastrointestinal tract and removes it from the body through feces. It has the same effect and indication as sevelamer, but it also provides calcium supplementation. However, it is not an urgent issue in AKI, and it does not affect the potassium level.
Choice D reason: Epoetin alfa, recombinant is a medication that stimulates the production of red blood cells in the bone marrow. It is used to treat anemia, which is a low level of hemoglobin or red blood cells in the blood. Anemia can cause fatigue, weakness, and shortness of breath, and it is a common complication of CKD and AKI. However, it is not an urgent issue in AKI, and it does not affect the potassium level.
Correct Answer is ["F","H"]
Explanation
a) Basic metabolic panel: This is a blood test that measures the levels of electrolytes, glucose, calcium, and kidney function. It is not a priority order for this client because her glucose level is within the normal range and her symptoms are not indicative of electrolyte imbalance or kidney failure.
b) Echocardiogram: This is a test that uses sound waves to create images of the heart and its valves, chambers, and blood flow. It is not a priority order for this client because her chest discomfort may not be related to a cardiac problem and her SpO2 is normal, indicating adequate oxygenation.
c) CT scan of abdomen: This is a test that uses X-rays to create detailed pictures of the organs and structures in the abdomen. It is not a priority order for this client because her abdominal pain is not severe or acute and her nausea and poor appetite may be due to her illness or dialysis.
d) Blood cultures times 2 sets: This is a test that checks for the presence of bacteria or fungi in the blood. It is not a priority order for this client because she does not have signs of infection such as fever, chills, or leukocytosis.
e) Chest X-ray: This is a test that uses X-rays to create images of the lungs and chest wall. It is not a priority order for this client because she does not have respiratory symptoms such as cough, shortness of breath, or wheezes.
f) Place on continuous cardiac monitor: This is an order that requires the nurse to attach electrodes to the client's chest and monitor the heart rate and rhythm continuously. This is a priority order for this client because she has a history of CAD and HTN and reports chest discomfort and lightheadedness, which could indicate a possible myocardial infarction (heart attack) or arrhythmia (irregular heartbeat).
g) CBC: This is a blood test that measures the number and types of blood cells, such as red blood cells, white blood cells, and platelets. It is not a priority order for this client because she does not have signs of anemia, bleeding, or infection.
h) 12 lead EKG: This is a test that records the electrical activity of the heart from 12 different angles. It can detect abnormalities in the heart's rhythm, conduction, or damage. This is a priority order for this client because she has a history of CAD and HTN and reports chest discomfort and lightheadedness, which could indicate a possible myocardial infarction (heart attack) or arrhythmia (irregular heartbeat).
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today