The nurse understands that certain patients are more susceptible to pressure ulcer development. Which clients should the nurse identify as being at an increased risk for this health problem? Select all that apply.
Client with restricted activity
Client who can ambulate
Client with a cast
Client with good nutrition
Client with urinary and fecal incontinence
Correct Answer : A,C,E
A. Client with restricted activity - Patients with limited mobility are at a higher risk for pressure ulcers because they are unable to change positions easily, leading to prolonged pressure on certain body parts.
B. Client who can ambulate - Patients who can ambulate have the ability to shift their body weight and change positions, reducing the risk of prolonged pressure on specific areas. Ambulation can improve circulation and reduce the risk of pressure ulcers
C. Client with a cast - Clients with casts are often limited in their ability to move or change positions, making them susceptible to pressure ulcers in areas where the cast creates pressure points on the skin.
D. Client with good nutrition - Proper nutrition is essential for overall health, including skin health. Adequate nutrition promotes wound healing and tissue repair. Good nutrition is not a risk factor for pressure ulcers; in fact, it can contribute to preventing them by maintaining healthy skin.
E. Client with urinary and fecal incontinence - Incontinence can lead to moisture on the skin, making it more susceptible to breakdown. Prolonged exposure to moisture, especially in the presence of urine or feces, can increase the risk of pressure ulcer development.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
A. Apply a moisture barrier ointment to the client's skin
Applying a moisture barrier ointment creates a protective barrier on the skin, preventing prolonged exposure to moisture, which can lead to skin breakdown in individuals with urinary incontinence. Keeping the skin dry and protected is essential in preventing skin irritation and breakdown.
B. Check the client's skin every 8 hr for signs of breakdown - Skin should be assessed more frequently, ideally every 2-4 hours, especially in clients with urinary incontinence, to detect signs of breakdown early.
C. Clean the client's skin and perineum with hot water after each episode of incontinence - Hot water can be harsh on the skin and exacerbate irritation. It's recommended to use mild, warm water and gentle cleansing techniques. Harsh cleaning methods can damage the skin.
D. Request a prescription for the insertion of an indwelling urinary catheter - Indwelling urinary catheters pose an increased risk of infection and other complications. Catheters should only be used when absolutely necessary, and preventive measures should be taken to manage incontinence without catheterization whenever possible.
Correct Answer is B
Explanation
A. Morse Scale:
The Morse Scale, also known as the Morse Fall Scale, is used to assess a patient's risk of falling. It evaluates various factors such as history of falling, secondary diagnosis, ambulatory aids, IV therapy, gait, and mental status. It is primarily focused on assessing the risk of falls, not pressure ulcers.
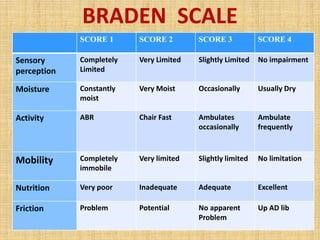
B. Braden Scale:
As previously mentioned, the Braden Scale assesses a patient's risk for developing pressure ulcers. It takes into account sensory perception, moisture, activity, mobility, nutrition, and friction/shear. The scale helps healthcare providers determine the level of risk a patient has for developing pressure sores and guides interventions to prevent them.
C. Bristol Scale:
The Bristol Stool Scale is used to classify the form of human feces into seven categories. It is a medical aid designed to classify the form of human feces into seven categories. This scale is primarily used to assess bowel movements and is unrelated to pressure ulcers.
D. Hendrich II Scale:
The Hendrich II Fall Risk Model is a tool designed to identify patients at risk for falls. It includes factors such as confusion, symptomatic depression, altered elimination, dizziness, male gender, and the use of antiepileptics, benzodiazepines, or non-opioid analgesics. Similar to the Morse Scale, it focuses on assessing the risk of falls, not pressure ulcers.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today