The practical nurse (PN) is assessing an older client with left-sided heart failure (HF). What intervention is most important for the PN to implement?
Inspect for sacral edema.
Measure urinary output.
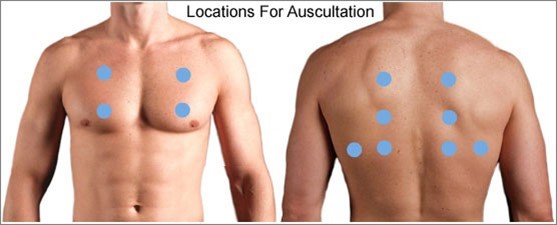
Auscultate all lung fields.
Check mental acuity.
The Correct Answer is C
When assessing an older client with left-sided heart failure (HF), the most important intervention for the practical nurse (PN) to implement is to auscultate all lung fields. Left-sided heart failure is characterized by the inability of the left ventricle to effectively pump blood, leading to fluid accumulation in the lungs. Auscultating all lung fields allows the PN to assess for the presence of abnormal lung sounds such as crackles, indicating pulmonary congestion.
Let's evaluate the other options:
a) Inspect for sacral edema.
Sacral edema is commonly associated with right-sided heart failure, not left-sided heart failure. While it is important to assess for edema in clients with heart failure, inspecting for sacral edema may not be the most immediate and crucial intervention in this specific case.
b) Measure urinary output.
Measuring urinary output is a valuable assessment in many clinical situations, but it may not be the most vital intervention in the context of left-sided heart failure. Monitoring urinary output is more relevant in assessing kidney function and fluid balance rather than directly assessing the severity of left-sided heart failure.
d) Check mental acuity.
Checking mental acuity is important in assessing the overall condition of the client, but it is not the most crucial intervention specifically related to left-sided heart failure. Mental status evaluation is more useful in identifying signs of altered mental status or potential complications, rather than directly assessing the impact of left-sided heart failure.
In summary, when assessing an older client with left-sided heart failure, the most important intervention for the practical nurse (PN) to implement is to auscultate all lung fields. This allows for the detection of abnormal lung sounds associated with pulmonary congestion, a hallmark sign of left-sided heart failure.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
Choice D rationale:
Taking zolpidem before bedtime is the correct information to include in the education. Zolpidem is a medication used for the short-term treatment of insomnia and should be taken immediately before going to bed to facilitate sleep onset.
Choice A rationale:
Crushing zolpidem to increase absorption is not recommended. The medication should be taken whole and not crushed or chewed.
Choice B rationale:
Storing zolpidem at room temperature is correct. Like many medications, zolpidem should be stored at a controlled room temperature, away from moisture and heat.
Choice C rationale:
Administering zolpidem with a meal is not necessary and may delay the onset of its effects. It is typically taken on an empty stomach for faster absorption.
Correct Answer is D
Explanation
The correct answer is D. Notify your healthcare provider if you start having abdominal pain.
Choice A rationale:
Exenatide does not act in the same way as insulin. Insulin directly lowers blood glucose levels by facilitating the uptake of glucose into cells, while exenatide is an incretin mimetic that enhances glucose-dependent insulin secretion and slows gastric emptying.
Choice B rationale:
Exenatide should be injected within 30 minutes before or after a meal, but this is not the most critical information for discharge instructions.
Choice C rationale:
There are precautions about taking exenatide with other medications, especially those that affect kidney function or interact with exenatide.
Choice D rationale:
Notifying the healthcare provider if abdominal pain starts is crucial because exenatide can cause side effects such as pancreatitis, which presents with severe abdominal pain. Early detection and intervention are essential for patient safety.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today