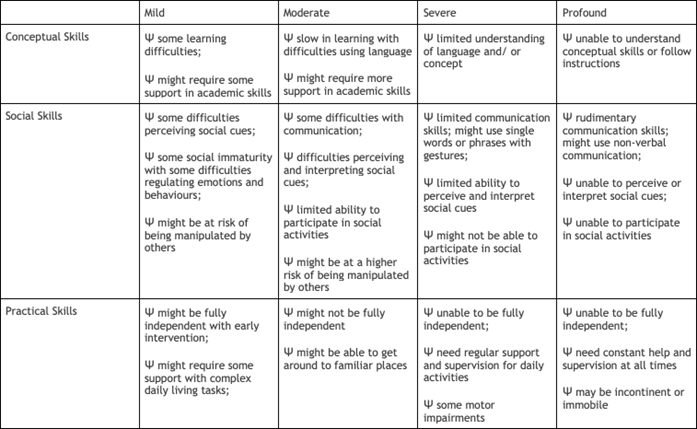
The practical nurse (PN) is caring for a 4-year-old girl with a moderate developmental disability. Which is the primary goal of treatment for a child with a developmental disability?
Help the child achieve maximum potential.
Meet the child's rehabilitation needs.
Help prevent further disability.
Promote the child's social acceptability.
The Correct Answer is A
The primary goal of treatment for a child with a developmental disability is to help the child reach their full potential, despite their disability. This involves identifying and addressing any barriers to the child's development and providing them with the necessary support and interventions to promote their growth and development. It is important to focus on the child's abilities and strengths rather than their limitations.
Option B is incorrect as it focuses on rehabilitation, which is not the primary goal of treatment for a child with a developmental disability.
Option C is incorrect as it refers to preventing further disability, which may not always be possible depending on the cause of the disability.
Option D is incorrect as it focuses on social acceptability, which is not the primary goal of treatment for a child with a developmental disability.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
The fact that the patient is being treated for depression and is currently taking an antidepressant medication suggests that his loss of interest in sexual intimacy may be related to his medication. Certain antidepressants can cause sexual dysfunction, including decreased libido.
Therefore, obtaining a list of medications currently being taken (A) is the most important information for the PN to obtain. While marital discord (B), frequency of sexual activity (C), and alcohol consumption (D) may be relevant information, they are not as directly related to the patient's current complaint as his medication use.
Correct Answer is A
Explanation
During pregnancy, it is important for the client to consume a balanced and nutritious diet that includes adequate protein, vitamins, and minerals. However, clients with nausea and vomiting may have difficulty tolerating certain foods, particularly those that are high in fat or spicy. Cheeseburgers and French fries are typically high in fat and can exacerbate nausea, making them a poor choice for a client with this symptom.
Baked chicken with rice and pasta with steamed vegetables are both healthier options that can provide the client with adequate nutrition.
Baked potato chips and lemonade may be a suitable snack for some clients, but the high salt content of the chips may exacerbate fluid retention, which can be a concern for clients with pyelonephritis. The PN should encourage the client to choose healthier options and avoid foods that are likely to exacerbate her symptoms.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today