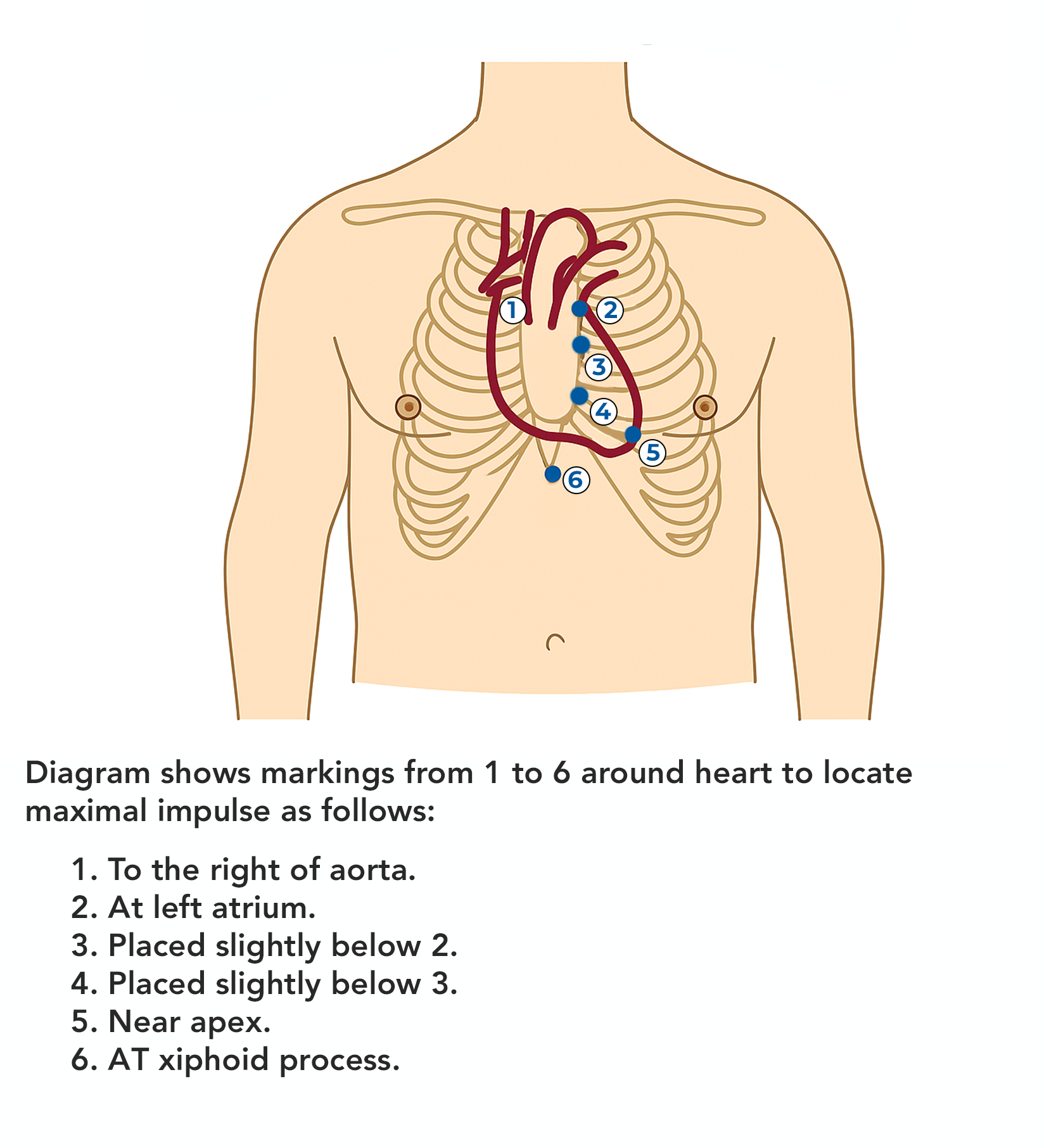
Which number marks the location where the nurse would auscultate the point of maximal impulse (PMI)?
1
2
3
4
5
The Correct Answer is A
The Point of Maximal Impulse (PMI), also referred to as the apical impulse, is the location on the chest wall where the heartbeat is most strongly felt or heard. It corresponds to the apex of the heart, typically located at the 5th intercostal space, midclavicular line in adults
Rationale for correct answers:
E. Near apex: This point corresponds to the 5th intercostal space at the midclavicular line, where the apex of the heart contacts the chest wall. It is the most accurate site for auscultating the apical pulse and evaluating left ventricular function.
Rationale for incorrect answers:
A. To the right of the aorta. This is in the right upper sternal border, typically used to auscultate the aortic valve area. It is not associated with the PMI or apex of the heart.
B. At left atrium: This is positioned more posteriorly in the chest and not palpable or auscultated directly from the anterior chest wall.
C. Placed slightly below 2: Still in the left parasternal area, likely over the pulmonic or tricuspid area, but not the apex.
D. Placed slightly below 3: This is near the left lower sternal border, where tricuspid sounds may be heard, but it's still not the apex.
F. At xiphoid process: This is the epigastric area, well below the heart’s apex, and is not used to assess apical pulse or PMI.
Take-home points:
- The PMI is best auscultated at the 5th intercostal space, midclavicular line, which corresponds to point 5 in the diagram.
- Accurate location of the PMI is essential in assessing left ventricular function and detecting cardiac enlargement or displacement.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Vital signs provide critical information about a client's physiological status. When evaluating temperature, it's essential to consider normal ranges, the client’s baseline, and potential factors affecting the measurement (e.g., equipment error, recent food or fluid intake).
Rationale for correct answer:
B. Check what the client’s temperature was the last time it was taken: A single temperature reading may be normal or abnormal depending on the client's baseline pattern. Comparing previous readings helps determine whether this value is consistent or a new finding that might warrant further assessment.
Rationale for incorrect answers:
A. Wait 15 minutes and retake it: There is no indication that the initial temperature was affected by recent activity such as eating, drinking, or smoking, which could temporarily alter an oral temperature.
C. Retake it using a different thermometer: There’s no indication that the equipment is malfunctioning. If the reading had been inconsistent with the client’s condition, or if the thermometer showed an error, retaking with a different device would be reasonable.
D. Chart the temperature; it is normal: While 3F.1°C (97.2°F) is technically within the lower limit of normal, this option skips an important clinical validation step: checking for trends. The nurse may miss a developing pattern of hypothermia or a declining trend in temperature.
Take-home points:
- Always compare current vital signs with the client’s baseline and trends to determine clinical significance.
- Low-normal temperature readings require context- never assume they're acceptable without reviewing previous data and clinical presentation.
Correct Answer is ["C","D","E"]
Explanation
In clients who have had a stroke, especially those with facial drooping, dysphagia (difficulty swallowing), or immobility, the nurse must choose a method of taking temperature that minimizes risk (e.g., aspiration or injury) and provides consistent, accurate readings.
Rationale for correct answer:
C. Axillary: Safe, noninvasive, and easy to perform even in clients with limited mobility. While it is less accurate than core sites, it’s a reasonable alternative when oral and rectal sites are contraindicated.
D. Tympanic: Quick, noninvasive, and reflects core temperature well. Not affected by oral or facial dysfunctions. Can be performed even when the client has limited cooperation.
E. Temporal artery: Noninvasive, fast, and generally well tolerated. Can be used in immobile or neurologically impaired clients without requiring cooperation.
Rationale for incorrect answers:
A. Oral: Oral temperature measurement requires the client to close their mouth tightly around the probe, which is compromised by facial drooping and dysphagia.
B. Rectal: While rectal temperature is accurate, it is invasive and can be uncomfortable, particularly in older or immobile clients.
Take-home points:
- Avoid oral and rectal routes in clients with neurologic deficits, swallowing issues, or limited mobility due to safety concerns.
- Axillary, tympanic, and temporal artery methods are safe, noninvasive, and appropriate for clients with stroke-related impairments.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today