
Hesi RN Fundamentals of Nursing Proctored Exam
Hesi RN Fundamentals of Nursing Proctored Exam
Total Questions : 43
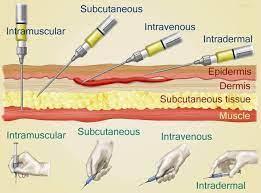
Showing 10 questions Sign up for moreThe nurse is teaching a client how to self-administer low-molecular-weight heparin subcutaneously. Which instruction should the nurse include?
Explanation
Choice A Reason: Massaging the injection site can cause bruising and bleeding, and is not recommended for subcutaneous heparin injections.
Choice B Reason: Rotating injections between different body sites can increase the risk of hematoma formation and skin irritation, and is not advised for subcutaneous heparin injections.
Choice C Reason: Expelling the air in the prefilled syringe can result in a loss of medication dose, and is not necessary for subcutaneous heparin injections.
Choice D Reason: Injecting in the abdominal area at least 2 inches from the umbilicus is the correct technique for subcutaneous heparin injections, as it reduces the risk of injury to blood vessels and nerves, and ensures consistent absorption of the medication.
Patient Data
Based on the trending heart rate and pain score, what should the nurse do? Select all that apply.
Explanation
Choice A: Lead the client in guided imagery
This is a correct choice because guided imagery is a non-pharmacological intervention that can help reduce pain and anxiety by creating a relaxing mental image for the client. Guided imagery can also lower the heart rate and blood pressure by activating the parasympathetic nervous system.
Choice B: Give a dose of 2.5 mg of Morphine
This is an incorrect choice because morphine is an opioid analgesic that can cause respiratory depression, hypotension, and bradycardia. The client's heart rate is already elevated, which could indicate inadequate pain relief or anxiety. Giving more morphine could worsen the client's condition and mask the underlying cause of the pain.
Choice C: Assist the client to walk around the room
This is an incorrect choice because walking around the room could increase the client's pain and heart rate by stimulating the sympathetic nervous system. The client has already done ambulation exercises with physical therapy at 1200, so there is no need to repeat them at 1400. The client should be allowed to rest in bed and conserve energy.
Choice D: Assess for sources of pain other than the surgical site
This is a correct choice because the nurse should always assess the client holistically and rule out any other potential causes of pain, such as infection, inflammation, or ischemia. The nurse should also check the surgical site for any signs of bleeding, hematoma, or infection. The nurse should use a comprehensive pain assessment tool that includes the location, intensity, quality, duration, frequency, and aggravating and relieving factors of the pain.
Choice E: Consult with the surgeon about the pain level
This is a correct choice because the nurse should collaborate with the surgeon and other members of the health care team to provide optimal pain management for the client. The nurse should report the client's pain score, vital signs, medication administration, and response to interventions. The surgeon may order additional tests or medications to address the cause of the pain and improve the client's comfort.
The nurse is caring for a client who is postoperative and receiving supplemental oxygen at 2 L/minute via nasal cannula. The oxygen saturation is 89%. Which action should the nurse implement?
Explanation
Choice A reason: Switching to a non-rebreather mask is not the immediate action to take. Non-rebreather masks deliver a high concentration of oxygen, typically reserved for severe hypoxia. The patient’s oxygen saturation is low, but not critically low. It’s important to first ensure the accuracy of the reading before escalating oxygen delivery methods.
Choice B reason: Removing the nasal cannula is not advisable. The patient is postoperative and may have impaired gas exchange due to anesthesia, pain, or decreased mobility. Removing the supplemental oxygen may worsen the patient’s hypoxemia and increase the risk of complications.
Choice C reason: Increasing the oxygen to 3 L/minute could be a potential action if the oxygen saturation reading is accurate and the patient’s condition does not improve. However, any changes to a patient’s oxygen therapy should be made under the guidance of a healthcare provider. It’s important to first verify the accuracy of the oxygen saturation reading.
Choice D reason: Verifying the placement of the pulse oximeter is the highest priority action. Before making changes to the oxygen flow rate, it’s important to ensure that the oxygen saturation reading is accurate. Incorrect placement or function of the pulse oximeter could lead to inaccurate readings.
Which assessment is most important for the nurse to perform prior to the application of a heating pad?
Explanation
Choice A: Limitations to range of motion are not directly related to the application of a heating pad. A heating pad may help reduce pain and stiffness, but it does not affect the range of motion itself.
Choice B: Muscle strength and tone are also not directly related to the application of a heating pad. A heating pad may relax tense muscles, but it does not affect the strength or tone of the muscles.
Choice C: Degree of neurosensory impairment is the most important assessment for the nurse to perform prior to the application of a heating pad. A heating pad can cause burns or tissue damage if the patient has impaired sensation and cannot feel the heat or pain. The nurse should check the patient's ability to perceive temperature, pressure, and pain before applying a heating pad.
Choice D: Presence of rebound phenomenon is not relevant to the application of a heating pad. Rebound phenomenon refers to the worsening of symptoms after discontinuing a medication or treatment. A heating pad does not cause rebound phenomenon.
After an intravenous antibiotic is started, the nurse determines that the medication is not prescribed for the client and stops the infusion. Which action should the nurse implement next?
Explanation
Choice A: Notify the healthcare provider is the correct action because it is the nurse's responsibility to report any medication errors or adverse reactions to the prescriber as soon as possible.
Choice B: Document the event on the chart is not the next action because it should be done after notifying the healthcare provider and completing an incident report.
Choice C: Complete an incident report is not the next action because it should be done after notifying the healthcare provider and before documenting the event on the chart.
Choice D: Inform the nurse on the next shift is not the next action because it should be done after documenting the event on the chart and during handoff.
A hospitalized client who has an advance directive and healthcare power of attorney is receiving enteral nutrition through a nasogastric (NG) tube. The client vomits and appears to be choking. Which action should the nurse take?
Explanation
The correct answer is: d. Perform oropharyngeal suctioning.
Choice A: Irrigate the nasogastric tube with water
Reason: Irrigating the nasogastric tube with water is not appropriate when a client is choking and vomiting. This action could potentially worsen the situation by introducing more fluid into the stomach, increasing the risk of aspiration.
Choice B: Review the advance directive document
Reason: Reviewing the advance directive document is not an immediate action to take when a client is choking. Advance directives provide guidance on the client’s wishes for medical treatment but do not address acute emergency interventions.
Choice C: Elevate the head of bed 45 degrees
Reason: Elevating the head of the bed to 45 degrees can help reduce the risk of aspiration by using gravity to keep stomach contents down. However, this action alone is not sufficient to address the immediate choking hazard.
Choice D: Perform oropharyngeal suctioning
Reason: Performing oropharyngeal suctioning is the correct action because it directly addresses the choking hazard by clearing the airway of vomit and other obstructions. This is a critical step to ensure the client’s airway is clear and they can breathe properly.
A client with a family history of cardiac disease is seeking information to control risk factors. Which lifestyle modification is most important for the nurse to encourage?
Explanation
Choice A: Regular exercise is a good lifestyle modification, but it is not as important as smoking cessation. Exercise can help lower blood pressure, cholesterol, and weight, but it cannot reverse the damage caused by smoking.
Choice B: Stress reduction is a good lifestyle modification, but it is not as important as smoking cessation. Stress can trigger or worsen cardiac problems, but it cannot cause them as directly as smoking.
Choice C: Smoking cessation is the most important lifestyle modification because smoking is a major risk factor for cardiac disease. Smoking damages the blood vessels, increases blood pressure, reduces oxygen supply, and promotes clot formation.
Choice D: Low-fat diet is a good lifestyle modification, but it is not as important as smoking cessation. A low-fat diet can help lower cholesterol and prevent plaque buildup, but it cannot undo the effects of smoking.
The nurse observes a decrease in a client's level of consciousness. Which vital sign should the nurse obtain first?
Explanation
Choice A: Blood pressure is not the first vital sign to obtain because it is not as sensitive to changes in the level of consciousness as respiratory rate. Blood pressure may be normal or elevated in some cases of decreased consciousness, such as stroke or head injury.
Choice B: Temperature is not the first vital sign to obtain because it is not as relevant to the level of consciousness as respiratory rate. Temperature may be normal or slightly elevated in some cases of decreased consciousness, such as infection or dehydration.
Choice C: Respiratory rate is the first vital sign to obtain because it reflects the adequacy of oxygenation and ventilation, which are essential for brain function. Respiratory rate may be increased, decreased, or irregular in cases of decreased consciousness, depending on the cause and severity.
Choice D: Pulse rate is not the first vital sign to obtain because it is not as indicative of the level of consciousness as respiratory rate. Pulse rate may be normal, fast, or slow in cases of decreased consciousness, depending on the cause and compensatory mechanisms.
Patient Data
Review H and P and nurse's notes.
Identify from the choices area to specify which condition the client is most likely experiencing, two actions the nurse should take to address that condition, and two parameters the nurse should monitor to assess the client's progress.
Explanation
Potential Conditions
Overflow urinary incontinence
This is the correct choice because overflow urinary incontinence is the involuntary loss of urine due to a distended bladder that cannot empty completely. The client has cerebral palsy, which can affect the bladder muscles and nerves, causing them to lose coordination and contractility. The client is also non-verbal and has severe intellectual disability, which can impair his ability to sense or communicate the need to void. The client's clothes and sheets are wet, indicating that he has leaked urine. The client voided approximately 75 mL of urine, which is a small amount for an adult male. These signs suggest that the client has overflow urinary incontinence.
Actions to Take
Provide skin care
This is a correct choice because the nurse should provide skin care to the client who has overflow urinary incontinence. The nurse should cleanse the perineal area with mild soap and water, pat dry, and apply a barrier cream or ointment to protect the skin from moisture and irritation. The nurse should also change the client's clothes and sheets as needed to keep him dry and comfortable.
Place an incontinence containment product under the client
This is a correct choice because the nurse should place an incontinence containment product under the client who has overflow urinary incontinence. An incontinence containment product is a device or material that absorbs or collects urine, such as a diaper, pad, or catheter. The nurse should choose an appropriate product based on the client's preferences, needs, and abilities. The nurse should also monitor the product for leakage, odor, or infection, and change it regularly.
Parameters to Monitor
Intake and output
This is a correct choice because the nurse should monitor the intake and output of the client who has overflow urinary incontinence. The nurse should measure and record the amount and type of fluids that the client consumes and excretes. The nurse should also note the color, clarity, odor, and specific gravity of the urine. The nurse should compare the intake and output with the normal ranges for the client's age, weight, and condition. The nurse should report any abnormal findings or changes to the health care provider.
Post-void residual
This is a correct choice because the nurse should monitor the post-void residual of the client who has overflow urinary incontinence. Post-void residual is the amount of urine left in the bladder after voiding. The nurse can measure it by using a bladder scanner or inserting a catheter after the client voids. A normal post-void residual is less than 50 mL for an adult male. A high post-void residual indicates that the bladder is not emptying completely, which can lead to overflow urinary incontinence. The nurse should report any high post-void residual to the health care provider.
A client who had surgery 3 days ago is sitting with head of bed at 75 degrees and requests to be repositioned. Which instruction is most important for the nurse to provide to the unlicensed assistive personnel (UAP)?
Explanation
Choice A: Have the client hold a pillow over the abdomen to cough and deep breathe is not the most important instruction because it is not related to repositioning. This is a good practice to prevent respiratory complications after surgery, but it can be done at any time.
Choice B: Encourage the client to eat all of the meals that are sent is not the most important instruction because it is not related to repositioning. This is a good practice to promote nutrition and healing after surgery, but it can be done at any time.
Choice C: Offer fruit juice at least twice during both the day and evening shifts is not the most important instruction because it is not related to repositioning. This is a good practice to prevent dehydration and constipation after surgery, but it can be done at any time.
Choice D: Lower the bed prior to helping the client to move up in bed is the most important instruction because it reduces the risk of injury and falls for both the client and the UAP. This is a safety measure that should be done before any repositioning.
You just viewed 10 questions out of the 43 questions on the Hesi RN Fundamentals of Nursing Proctored Exam Exam. Subscribe to our Premium Package to obtain access on all the questions and have unlimited access on all Exams. Subscribe Now

