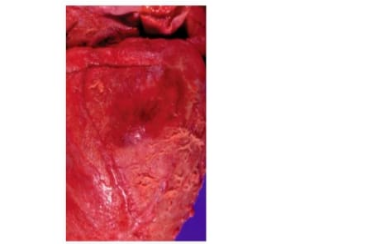
A 55-year-old man with polycystic kidney disease dies in renal failure (uremia). A shaggy exudate on the surface of this heart is observed at autopsy (shown). This inflammatory exudate contains large amounts of which of the following plasma-derived proteins?
Albumin
Fibrin
Fibronectin
Plasmin
Thrombin
The Correct Answer is B
A. Albumin: Albumin is the most abundant plasma protein and primarily maintains oncotic pressure and transports molecules. It is not a structural component of the fibrinous exudate seen in pericarditis.
B. Fibrin: Fibrin is a key plasma-derived protein formed from fibrinogen during the coagulation cascade. In fibrinous pericarditis, increased vascular permeability allows plasma proteins, particularly fibrinogen, to leak into the pericardial space, where it polymerizes into fibrin. This forms the characteristic “shaggy” or “bread-and-butter” appearance on the heart surface.
C. Fibronectin: Fibronectin is an extracellular matrix glycoprotein involved in tissue repair and cell adhesion. While it may play a minor role in wound healing, it is not the primary protein responsible for the gross fibrinous exudate in pericarditis.
D. Plasmin: Plasmin is a fibrinolytic enzyme that breaks down fibrin clots. It regulates clot dissolution but is not the structural protein forming the fibrinous exudate.
E. Thrombin: Thrombin is a protease that converts fibrinogen to fibrin during coagulation. While it initiates fibrin formation, the exudate itself is composed of fibrin polymers rather than thrombin.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
A. Congestive heart failure:Congestive heart failure can cause dyspnea and pulmonary congestion, but hemoptysis and sudden pleuritic chest pain are not classic presenting features. CHF-related pulmonary edema usually produces pink, frothy sputum rather than frank blood and develops in the context of volume overload rather than acute embolic events.
B. Cor pulmonale:Cor pulmonale refers to right ventricular hypertrophy and failure secondary to chronic pulmonary hypertension. It develops gradually in patients with chronic lung disease and presents with peripheral edema and fatigue, not sudden chest pain and hemoptysis.
C. Phlebothrombosis:Phlebothrombosis refers to thrombus formation in a vein, often in the lower extremities, especially in patients with varicose veins. While it is the underlying source of emboli, it does not directly cause chest pain or hemoptysis unless a clot dislodges and travels to the lungs.
D. Pulmonary thromboembolism:Pulmonary thromboembolism occurs when a thrombus, often originating from deep leg veins, embolizes to the pulmonary arteries. Sudden chest pain and hemoptysis result from pulmonary infarction and pleural irritation. Varicose veins increase venous stasis, predisposing to thrombosis and subsequent embolism.
E. Pulmonary edema:Pulmonary edema involves fluid accumulation in the alveoli, most commonly due to left-sided heart failure. It causes dyspnea and crackles but does not typically present with sudden pleuritic chest pain and hemoptysis linked to venous thromboembolic risk factors.
Correct Answer is E
Explanation
A. Bacterial pneumonia:Bacterial pneumonia can cause dyspnea and rales, but it typically presents with fever, localized infiltrates on imaging, and productive cough. In this patient, the acute onset following extensive burns points toward non-infectious pulmonary injury rather than a primary bacterial infection.
B. Cardiogenic shock:Cardiogenic shock results from acute cardiac pump failure, leading to hypotension and poor organ perfusion. While pulmonary edema may accompany cardiogenic shock, there is no indication in this scenario that the patient has primary cardiac dysfunction; the burns and systemic inflammatory response are the key factors.
C. Congestive heart failure:Congestive heart failure causes pulmonary congestion and rales due to left ventricular dysfunction. This patient’s diffuse alveolar damage is a direct result of burn-induced systemic inflammation rather than chronic or acute cardiac failure, making CHF less likely.
D. Dehydration (hypovolemic shock):Hypovolemic shock from fluid loss in burns leads to low blood pressure and poor tissue perfusion. It does not cause pulmonary edema or alveolar rales, which are related to fluid accumulation in the lungs rather than intravascular volume depletion.
E. Pulmonary edema:Diffuse alveolar damage from burn injuries increases alveolar-capillary permeability, allowing protein-rich fluid to accumulate in alveoli. This results in pulmonary edema, causing rales on auscultation and dyspnea due to impaired gas exchange, making it the most likely cause of the patient’s respiratory findings.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today