A charge nurse in a long-term care facility is preparing an educational program about delirium for newly hired nurses. Which of the following statements should the nurse plan to Include?
"Delirium has an abrupt onset.”
"Delirium does not affect a client's perception of her environment."
"Delirium has a slow progression.”
Delirium does not affect a client's sleep cycle
The Correct Answer is A
Delirium is an acute confusional state that develops rapidly over a short period of time, often within hours or days. It is characterized by a disturbance in consciousness and attention, along with changes in cognition and perception.
Delirium can significantly impact a client's perception of their environment. Clients with delirium may experience hallucinations, delusions, and misinterpretations of their surroundings. They may become disoriented, have difficulty recognizing familiar people or places, and exhibit altered levels of awareness and attention.
As mentioned earlier, delirium has an abrupt onset, meaning it develops rapidly. Delirium is usually a transient condition that fluctuates throughout the day, with symptoms varying in severity.
Delirium can disrupt a client's sleep-wake cycle. Clients with delirium may experience disturbances in their sleep patterns, such as difficulty falling asleep, frequent awakening during the night, or excessive sleepiness during the day.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
In general, the legal guardian or parent of the infant is usually required to sign the consent form. In the given options, the most appropriate individual to sign the consent form for the infant's surgery would be the infant's 17-year-old mother. In many jurisdictions, a parent under the age of 18 is still considered the legal guardian of their child and is authorized to make decisions on behalf of the infant. However, it is important to note that the specific legal requirements may
Correct Answer is D
Explanation
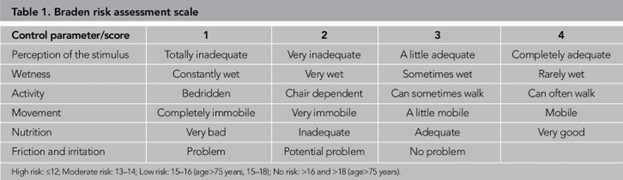
The Braden scale is a commonly used tool for assessing a patient's risk of developing pressure injuries (also known as pressure ulcers or bedsores). It evaluates six specific elements to determine the patient's risk level. These elements include sensory perception, moisture, activity, mobility, nutrition, and friction/shear. Each element is assessed and assigned a score, with a lower score indicating a higher risk for developing pressure injuries.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today