A client suffering from chronic obstructive pulmonary disease (COPD) reports that it is hard to cough up secretions and the secretions are thick and sticky. Which intervention will the nurse use to promote respiratory hygiene in this situation?
Decrease fluid intake.
Take Tylenol for the secretions.
Range -of-motion exercises as tolerated
Increase fluid intake.
The Correct Answer is D
Explanation: In clients with COPD, the secretions tend to be thick and sticky, which makes it difficult to cough up and clear the airway. To promote respiratory hygiene in this situation, the nurse should recommend increasing fluid intake. Adequate hydration helps to thin the secretions, making them easier to expectorate. The client should aim to drink at least 8-10 glasses of water or other fluids per day unless there is a medical reason not to do so.
Decreasing fluid intake (option a) would make the secretions even thicker and more difficult to clear. Taking Tylenol for secretions (option b) is not a recommended intervention as Tylenol is not indicated for thinning of secretions. Range-of-motion exercises (option c) are important to prevent complications such as pneumonia, but they are not directly related to promoting respiratory hygiene in this situation.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
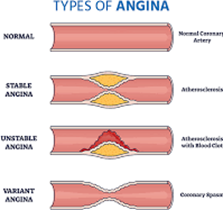
During exercise, the heart has to work harder to pump blood and oxygen to the muscles. In patients with stable angina, there is a partial blockage of the coronary arteries, which reduces blood flow and oxygen delivery to the heart muscle. This lack of oxygen to the heart muscles causes chest pain or discomfort, which subsides when the patient stops exercising and is relaxed.
Therefore, it is important for the patient with stable angina to avoid activities that trigger chest pain, take prescribed medications, and make lifestyle modifications to manage their condition.
Correct Answer is B
Explanation
Fluid retention is a common complication in heart failure, and monitoring the client's fluid status is crucial to manage the condition effectively. Daily weights are an essential component of monitoring fluid status and are the most sensitive and practical method to detect changes in the client's fluid status. Weight gain is a reliable indicator of fluid retention, and even small increases in weight can indicate the need for changes in the client's treatment plan.
Although electrolyte monitoring (option a), output measurements (option c), and daily BUN and serum creatinine monitoring (option d) can provide valuable information about the client's fluid status, they are not as sensitive or practical as daily weights. Electrolyte monitoring can help detect changes in fluid balance, but it does not provide a direct indication of fluid status. Output measurements can indicate fluid loss, but they do not provide an accurate assessment of fluid retention. BUN and serum creatinine monitoring can detect changes in renal function, but they are not specific to fluid status.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today