A client who is having burn debridement states, "You are the worst nurse I have ever seen. All you do is hurt me." Which of the following responses should the nurse make?
"That's a hurtful thing to say."
"Why would you say such a thing?"
"Well, that's your opinion."
"Tell me more about that."
The Correct Answer is D
Choice A Reason: This choice is incorrect because it reflects the nurse's feelings rather than focusing on the client's needs. Saying "That's a hurtful thing to say" may make the client feel guilty or defensive, and it does not address the underlying cause of the client's anger or frustration.
Choice B Reason: This choice is incorrect because it sounds accusatory and confrontational rather than empathetic and supportive. Asking "Why would you say such a thing?" may make the client feel judged or criticized, and it does not explore the client's feelings or concerns.
Choice C Reason: This choice is incorrect because it dismisses the client's feelings rather than acknowledging them. Saying "Well, that's your opinion" may make the client feel ignored or invalidated, and it does not show respect or compassion for the client.
Choice D Reason: This choice is correct because it invites the client to express their feelings and concerns rather than shutting them down. Saying "Tell me more about that" may make the client feel heard and understood, and it may help to identify the source of their anger or frustration. The nurse can then use therapeutic communication skills such as active listening, reflecting, clarifying, or validating to establish rapport and trust with the client.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
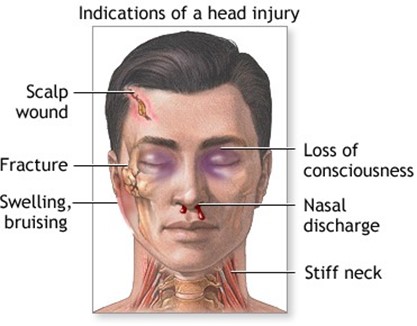
Choice A Reason: This is incorrect because the client is not unconscious, as the GCS score ranges from 3 to 15, with 3 being the lowest possible score and indicating deep coma or death.
Choice B Reason: This is correct because the client can follow simple motor commands, as the GCS score for best motor response is 5, which means the client can localize pain by moving his limbs away from the source of stimulation.To interpret the Glasgow Coma Scale (GCS) score provided in the scenario:Eye Opening (E): 3 - The client opens their eyes in response to verbal stimuli.Best Verbal Response (V): 5 - The client is oriented and able to engage in coherent conversation.Best Motor Response (M): 5 - The client can localize pain or follow motor commands (depending on additional context). The total GCS score would be 3 + 5 + 5 = 13, indicating a mild level of impairment or responsiveness.
Choice C Reason: This is incorrect because the client is able to make vocal sounds, as the GCS score for best verbal response is 5, which means the client can orient himself to person, place, and time.
Choice D Reason: This is incorrect because the client does not open his eyes when spoken to, as the GCS score for eye opening is 3, which means the client only opens his eyes in response to pain.
Correct Answer is A
Explanation
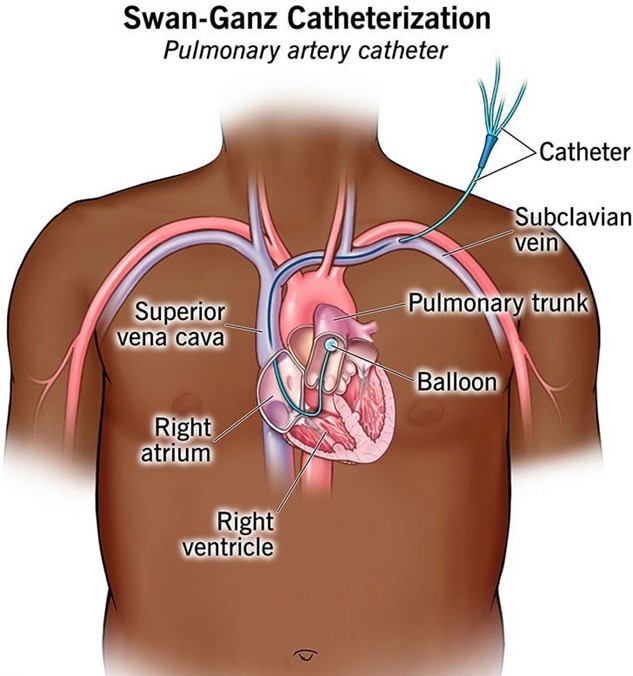
Choice A Reason: This is correct because a pulmonary artery catheter is a device that measures the pressures and flows in the heart and lungs, such as the pulmonary artery pressure, the pulmonary artery wedge pressure, the cardiac output, and the mixed venous oxygen saturation. These parameters reflect the hemodynamic status of the client, which is the balance between the cardiac output and the systemic vascular resistance.
Choice B Reason: This is incorrect because a pulmonary artery catheter does not measure spinal cord perfusion, which is the blood flow to the spinal cord. Spinal cord perfusion can be affected by spinal cord injury, spinal anesthesia, or spinal surgery.
Choice C Reason: This is incorrect because a pulmonary artery catheter does not measure renal function, which is the ability of the kidneys to filter waste products and maintain fluid and electrolyte balance. Renal function can be assessed by urine output, blood urea nitrogen, creatinine, and glomerular filtration rate.
Choice D Reason: This is incorrect because a pulmonary artery catheter does not measure intracranial pressure, which is the pressure inside the skull. Intracranial pressure can be increased by brain injury, stroke, tumor, infection, or hydrocephalus.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today