A client whose hyperthyroidism has not been responsive to medications is admitted for evaluation. During the admission assessment the client reports to the nurse of a sudden onset of feeling apprehensive and nurse notes the client is restless and very warm to touch. Which action should the nurse implement next?
Access laboratory results to confirm a thyroid crisis.
Obtain a complete set of vital signs.
Initiate intravenous access.
Encourage relaxation and slow deep breathing.
The Correct Answer is C
In this scenario, the client's sudden onset of feeling apprehensive, restlessness, and increased body temperature are consistent with symptoms of a thyroid crisis, also known as thyroid storm or thyrotoxic crisis. Thyroid crisis is a life-threatening condition that requires immediate medical intervention.
Initiating IV access is crucial to ensure the prompt administration of medications and fluids to manage the thyroid crisis effectively. IV access allows for the administration of beta-blockers, antithyroid drugs, and supportive care, which are essential components of the treatment for thyroid crisis. IV access also provides a route for fluid resuscitation if necessary.
Accessing laboratory results to confirm a thyroid crisis is important, but the clinical presentation of the client with sudden onset symptoms and a known history of uncontrolled hyperthyroidism suggests the need for immediate intervention rather than waiting for laboratory confirmation.
Obtaining a complete set of vital signs is an important assessment to gather comprehensive data, but in the case of a suspected thyroid crisis, immediate intervention takes precedence over obtaining vital signs.
Encouraging relaxation and slow deep breathing may be beneficial in managing anxiety or discomfort, but it does not address the underlying emergency situation of a thyroid crisis. The nurse should focus on initiating appropriate medical interventions first.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The correct answer is choice D. Demonstrate to the PN how to position the client more effectively for the procedure.
Choice A rationale:
Arranging for unlicensed assistive personnel to assist the PN during the procedure does not address the incorrect positioning of the client. The priority is to ensure the client is positioned correctly for the sigmoidoscopy, which is typically on the left side with knees drawn toward the chest.
Choice B rationale:
Acknowledging that the PN has positioned the client safely and correctly is not appropriate because the flat prone position is incorrect for a sigmoidoscopy. The correct position is on the left side with knees drawn toward the chest.
Choice C rationale:
Assuming care of the client and assigning the PN to the care of a different client does not address the educational opportunity. It is important to demonstrate the correct positioning to the PN to ensure proper care in future procedures.
Choice D rationale:
Demonstrating to the PN how to position the client more effectively for the procedure is the correct action. This ensures the client is in the proper position for the sigmoidoscopy and provides an educational opportunity for the PN.
Correct Answer is A
Explanation
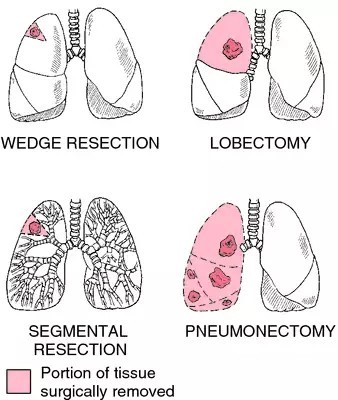
Following a pneumonectomy, it is important for the client to gradually resume normal activities and engage in social interactions. Encouraging family gatherings can provide emotional support, facilitate social connections, and help reduce feelings of isolation that the client may be experiencing.
While it is generally important for clients who have undergone a pneumonectomy to take precautions to reduce the risk of respiratory infections, such as avoiding crowded places and individuals with respiratory infections, completely avoiding social contact for several weeks is not necessary or realistic in most cases. It is essential to find a balance between protecting the client's health and promoting their emotional well-being and social integration.
Wearing a face mask during family events may not be necessary unless there is a specific concern about respiratory infections. The nurse can educate the client about the importance of good hand hygiene and avoiding close contact with individuals who are actively ill with respiratory infections.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today