A client with lung cancer who wears a subcutaneous morphine sulfate patch for pain is short of breath and is difficult to arouse. When performing a head to toe assessment, the nurse discovers four analgesic patches on the client's body. Which intervention should the nurse implement first?
Measure the client's blood pressure.
Remove all of the morphine patches.
Apply oxygen per face mask.
Administer a narcotic antagonist.
The Correct Answer is D
A. Measure the client's blood pressure:
While monitoring blood pressure is an important aspect of assessing a client's overall condition, it is not the immediate priority in a suspected opioid overdose. Respiratory depression and difficulty in arousing are more critical concerns that warrant prompt intervention with naloxone.
B. Remove all of the morphine patches:
While eventually, the nurse will need to address the presence of multiple morphine patches, removing them is not the first action. Administering naloxone to reverse the opioid effects takes precedence over patch removal.
C. Apply oxygen per face mask:
While providing oxygen may be necessary to support respiratory function, it doesn't address the underlying cause of the respiratory distress, which is likely opioid toxicity. Administering naloxone is the more direct and immediate intervention to counteract the effects of the opioids.
D. Administer a narcotic antagonist:
This is the correct and immediate priority. If the client is difficult to arouse and has multiple morphine patches, it raises concerns about opioid toxicity. Naloxone is a narcotic antagonist that can reverse the effects of opioid overdose, particularly respiratory depression, and is crucial in this scenario to restore normal respiratory function.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A. Evaluate upper and lower extremities for perfusion, pulse volume, and pitting edema:
This option focuses on assessing perfusion and circulation in the extremities. While it's important in certain situations, in the context of a client who recently underwent cardiac stent placement and is now experiencing chest pressure and shortness of breath, the priority is to assess the cardiac status more directly.
B. Listen for extra heart sounds, murmurs, and rhythm with the bell of the stethoscope:
This option involves auscultating the heart for abnormal sounds or rhythms. While it's a valuable assessment in general, in this particular scenario, obtaining an electrocardiogram (ECG) and initiating continuous cardiac monitoring would provide a more comprehensive and immediate evaluation of the cardiac status.
C. Obtain a 12-lead electrocardiogram and begin continuous cardiac monitoring:
This is the correct choice. Obtaining a 12-lead ECG and initiating continuous cardiac monitoring is crucial in assessing the client's cardiac function. It allows for the detection of any acute changes in the heart's electrical activity or rhythm, which is essential for timely intervention and management.
D. Verify troponin level assessments are scheduled every 3-6 hours for a series of three:
Monitoring troponin levels is important in assessing cardiac damage, but in this acute situation, obtaining an immediate ECG and initiating continuous cardiac monitoring take precedence for a more real-time evaluation of the client's cardiac status. Troponin levels may be monitored subsequently based on the initial findings.
Correct Answer is D
Explanation
A. Type 2 diabetes mellitus
Type 2 diabetes mellitus is not a contraindication for peritoneal dialysis. In fact, peritoneal dialysis can be a suitable option for individuals with diabetes who require renal replacement therapy. However, the presence of diabetes may require additional considerations and close monitoring.
B. Nephrotic syndrome history
Having a history of nephrotic syndrome is not a contraindication for peritoneal dialysis. Peritoneal dialysis can be used in individuals with various causes of chronic kidney disease, including those with nephrotic syndrome.
C. Latent hepatitis C
Latent hepatitis C alone may not be an absolute contraindication for peritoneal dialysis. However, the decision to initiate peritoneal dialysis would depend on the overall health status of the client, the degree of liver involvement, and the risk of infection. Close monitoring and appropriate precautions may be necessary.
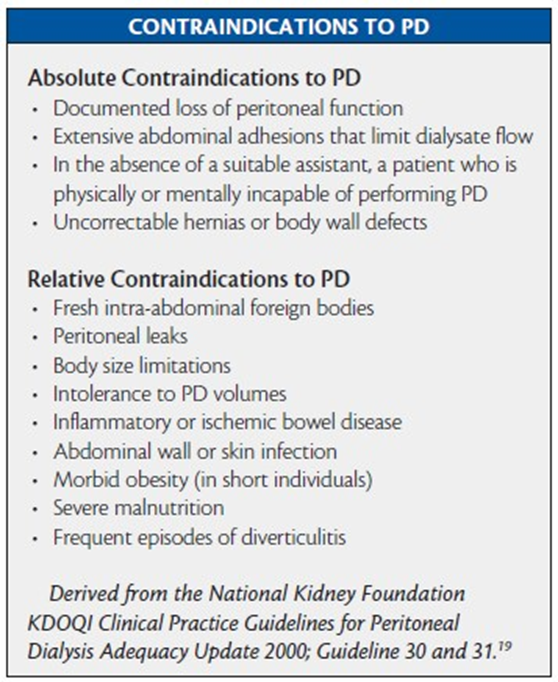
D. Crohn's disease with colectomy
Crohn's disease with colectomy is considered a contraindication for peritoneal dialysis. Surgical alterations in the abdomen, such as colectomy, can lead to adhesions or other complications that may interfere with the effectiveness of peritoneal dialysis. In such cases, alternative forms of dialysis, such as hemodialysis, may be considered.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today