A client with obsessive-compulsive disorder (OCD. is repeatedly washing the top of the same table. Which intervention should the nurse implement?
Encourage the client to be calm and relax for a while.
Teach the client thought-stopping techniques and how to refocus behaviors.
Assist the client to identify stimuli that precipitate the activity.
Allow time for the behavior and then redirect the client to other activities.
The Correct Answer is D
Choice D is correct because allowing time for the behavior and then redirecting the client to other activities is an effective intervention for a client with OCD who is repeatedly washing the top of the same table. OCD is a disorder characterized by recurrent and intrusive thoughts (obsessions) and repetitive and ritualistic behaviors (compulsions) that cause distress and impairment. The nurse should not interfere with or criticize the client's compulsions, as this can increase anxiety and resistance. The nurse should instead set limits on the time and place for the compulsions and gradually reduce them by offering alternative coping strategies or distractions.
Choice A is incorrect because encouraging the client to be calm and relax for a while is not an effective intervention for a client with OCD who is repeatedly washing the top of the same table. The client may not be able to relax or stop their compulsions, as they are driven by irrational fears or beliefs that are difficult to control. The nurse should not minimize or dismiss the client's feelings, as this can make them feel misunderstood or invalidated.
Choice B is incorrect because teaching the client thought-stopping techniques and how to refocus behaviors is not an effective intervention for a client with OCD who is repeatedly washing the top of the same table. Thought-stopping techniques are cognitive strategies that aim to interrupt or replace negative or unwanted thoughts with positive or neutral ones. However, these techniques may not work for clients with OCD, as their obsessions are often persistent and resistant to change. The nurse should not attempt to teach new skills or challenge the client's thoughts during an acute episode of compulsion, as this can increase anxiety and frustration.
Choice C is incorrect because assisting the client to identify stimuli that precipitate the activity is not an effective intervention for a client with OCD who is repeatedly washing the top of the same table. The client may not be able to identify or avoid the triggers that cause their compulsions, as they are often internal or irrational. The nurse should not focus on finding the cause or meaning of the compulsions, as this can reinforce their significance or validity.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
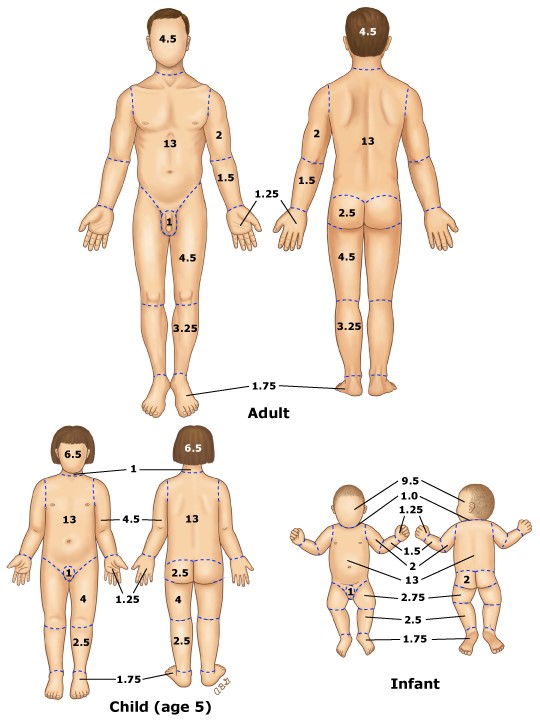
Choice A reason: This is the correct answer.According to the rule of nines, each leg accounts for 18% of the total body surface area, and the anterior surface of each leg accounts for half of that, or 9%. Therefore, the patient has partial-thickness burns on 9% + 9% = 18% of the body surface area.
Choice B reason: This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior and posterior surfaces of both legs, as well as the head and neck, which is not given in the question.
Choice C reason: This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior surface of only one leg, which is not given in the question.
Choice D reason: This is incorrect. This would be the case if the patient had partial-thickness burns on the anterior and posterior surfaces of both legs, which is not given in the question.
Correct Answer is D
Explanation
Choice A: Assessing pupillary response to light hourly is not an intervention that the nurse should implement while administering dopamine, as this is not related to the effects or side effects of dopamine. This is a distractor choice.
Choice B: Initiating seizure precautions is not an intervention that the nurse should implement while administering dopamine, as this is not a common or expected complication of dopamine. This is another distractor choice.
Choice C: Monitoring serum potassium frequently is not an intervention that the nurse should implement while administering dopamine, as this is not affected by dopamine or hypotension. This is another distractor choice.
Choice D: Measuring urinary output every hour is an intervention that the nurse should implement while administering dopamine, as this can indicate the effectiveness of dopamine in improving renal perfusion and blood pressure. Therefore, this is the correct choice.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today