A few weeks after an 82-year-old patient with a new diagnosis of type 2 diabetes has been placed on metformin (Glucophage) therapy and taught about appropriate diet and exercise, the home health nurse makes a visit. Which finding should the nurse promptly discuss with the health care provider?
Last eye examination was 18 months ago
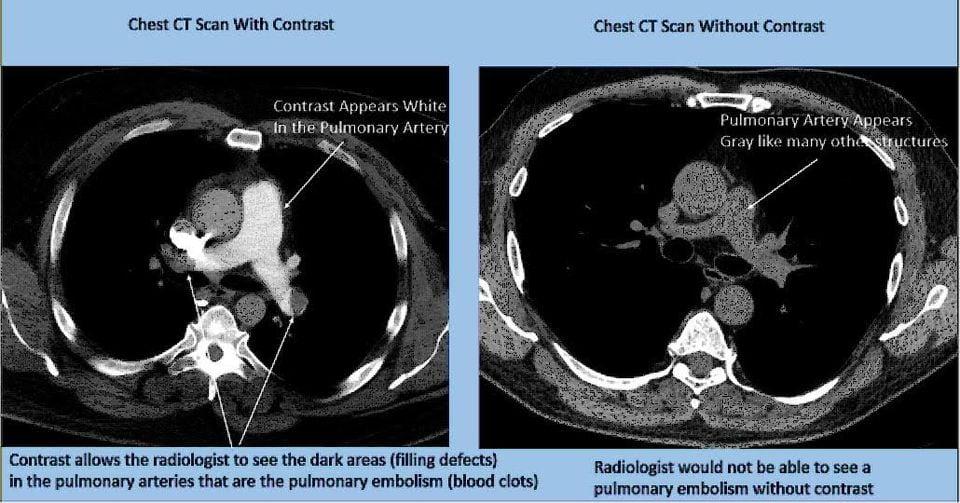
Patient states they are scheduled for a CT scan with contrast dye the next day
Hemoglobin A1C level is 7.9%
Patient has questions about the prescribed diet
The Correct Answer is B
Choice A reason: Last eye examination was 18 months ago is not a finding that requires immediate attention from the health care provider. However, the nurse should remind the patient of the importance of regular eye examinations, as diabetes can increase the risk of eye problems, such as cataracts, glaucoma, and diabetic retinopathy. The American Diabetes Association (ADA) recommends that patients with type 2 diabetes have a comprehensive eye examination at least once every two years¹.
Choice B reason: Patient states they are scheduled for a CT scan with contrast dye the next day is a finding that should be promptly discussed with the health care provider. Metformin is a medication that lowers the blood glucose level by reducing the liver's production of glucose and increasing the cells' sensitivity to insulin. Metformin can interact with contrast dye, which is a substance that is injected into the veins to enhance the visibility of organs and tissues in imaging tests, such as CT scans. Contrast dye can impair the kidney function and increase the risk of lactic acidosis, a rare but serious condition where the blood becomes too acidic due to the accumulation of lactic acid. Lactic acidosis can cause symptoms such as nausea, vomiting, abdominal pain, muscle weakness, and breathing difficulties. To prevent this complication, the ADA recommends that patients stop taking metformin at the time of or before the imaging procedure, and resume it 48 hours after the procedure, only if the kidney function is normal².
Choice C reason: Hemoglobin A1C level is 7.9% is not a finding that needs urgent discussion with the health care provider. Hemoglobin A1C is a test that measures the average blood glucose level over the past two to three months. It reflects how well the diabetes is controlled over time. The ADA recommends that most patients with type 2 diabetes aim for a hemoglobin A1C level of less than 7%, as this can reduce the risk of diabetes complications, such as heart disease, kidney disease, nerve damage, and eye damage. A hemoglobin A1C level of 7.9% indicates that the patient's blood glucose level is slightly above the target range, and may need some adjustment in the medication, diet, or exercise plan. However, this is not an emergency situation, and the nurse can review the patient's self-monitoring records, medication adherence, and lifestyle factors, and provide education and support as needed.
Choice D reason: Patient has questions about the prescribed diet is not a finding that warrants immediate communication with the health care provider. However, the nurse should address the patient's questions and concerns, and provide clear and consistent information about the dietary recommendations for type 2 diabetes. A healthy diet for type 2 diabetes should include a variety of foods, such as vegetables, fruits, whole grains, lean proteins, low-fat dairy, and healthy fats. The patient should also limit the intake of added sugars, refined carbohydrates, saturated fats, trans fats, and sodium. The nurse can help the patient plan their meals and snacks, and use tools such as carbohydrate counting, portion control, or the plate method to balance their food choices and blood glucose levels..
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason: 363 is not the correct answer. This is the daily maintenance fluid requirement for an infant who weighs 3.5 kg, not 16 kg. The formula for calculating the daily maintenance fluid requirement for infants who weigh between 3.5 and 10 kg is 100 mL/kg¹.
Choice B reason: 727 is not the correct answer. This is the daily maintenance fluid requirement for an infant who weighs 10 kg, not 16 kg. The formula for calculating the daily maintenance fluid requirement for infants who weigh between 10 and 20 kg is 1000 mL plus 50 mL for every kg over 10¹.
Choice C reason: 1300 is the correct answer. This is the daily maintenance fluid requirement for an infant who weighs 16 kg. The formula for calculating the daily maintenance fluid requirement for infants who weigh between 10 and 20 kg is 1000 mL plus 50 mL for every kg over 10¹. Therefore, for an infant who weighs 16 kg, the daily maintenance fluid requirement is 1000 mL plus 50 mL times 6, which equals 1300 mL.
Choice D reason: 1600 is not the correct answer. This is the daily maintenance fluid requirement for an infant who weighs 20 kg, not 16 kg. The formula for calculating the daily maintenance fluid requirement for infants who weigh between 10 and 20 kg is 1000 mL plus 50 mL for every kg over 10¹. For infants who weigh more than 20 kg, the formula is 1500 mL plus 20 mL for every kg over 20¹.
Correct Answer is B
Explanation
Choice A reason: Burning pain and tingling in extremities are not symptoms of autonomic neuropathy, but of peripheral neuropathy. Peripheral neuropathy affects the sensory and motor nerves that innervate the skin, muscles, and joints. It can cause pain, numbness, weakness, and loss of sensation in the extremities. Autonomic neuropathy affects the nerves that control the involuntary functions of the body, such as digestion, blood pressure, heart rate, and sweating.
Choice B reason: Nausea and feeling of abdominal fullness are symptoms of autonomic neuropathy, specifically of gastroparesis. Gastroparesis is a condition where the stomach muscles are weakened or paralyzed, and cannot move food properly. It can cause delayed gastric emptying, nausea, vomiting, bloating, early satiety, and poor blood glucose control. Autonomic neuropathy can damage the vagus nerve, which regulates the stomach motility and secretion.
Choice C reason: Elevated blood pressure and delayed capillary refill are not symptoms of autonomic neuropathy, but of cardiovascular problems. Blood pressure is the force of blood against the walls of the arteries, and capillary refill is the time it takes for the color to return to the nail bed after pressing on it. Elevated blood pressure can indicate hypertension, which is a risk factor for heart disease and stroke. Delayed capillary refill can indicate poor blood circulation, which can be caused by atherosclerosis, peripheral artery disease, or shock. Autonomic neuropathy can affect the blood pressure and heart rate, but usually causes hypotension and tachycardia, not hypertension and delayed capillary refill.
Choice D reason: Increased thirst and excessive urination are not symptoms of autonomic neuropathy, but of diabetes mellitus. Diabetes mellitus is a condition where the body cannot produce or use insulin properly, and the blood glucose level becomes too high. Increased thirst and excessive urination are signs of hyperglycemia, which is a high blood glucose level. Hyperglycemia can cause dehydration, electrolyte imbalance, and ketoacidosis. Autonomic neuropathy can be a complication of diabetes mellitus, but it does not cause increased thirst and excessive urination.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today