A nurse in a long-term care facility is collecting data from an older adult client. Which of the following findings indicates that the client might be dehydrated?
Recent onset of confusion
Cool, clammy skin
Decrease in pulse rate
Increase in blood pressure
The Correct Answer is A
Choice A: This is correct. Dehydration can cause electrolyte imbalance and affect the brain function, leading to confusion, dizziness, or lethargy.
Choice B: This is incorrect. Cool, clammy skin is a sign of shock, not dehydration. Dehydration can cause dry, warm skin.
Choice C: This is incorrect. Decrease in pulse rate is a sign of bradycardia, not dehydration. Dehydration can cause increase in pulse rate as the body tries to compensate for the low blood volume.
Choice D: This is incorrect. Increase in blood pressure is a sign of hypertension, not dehydration. Dehydration can cause decrease in blood pressure as the blood volume drops.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice C: Recommending consumption of cold items is an action that the nurse should take to help manage stomatitis, which is inflammation and ulceration of the oral mucosa. Cold items can help soothe the irritation and reduce swelling.
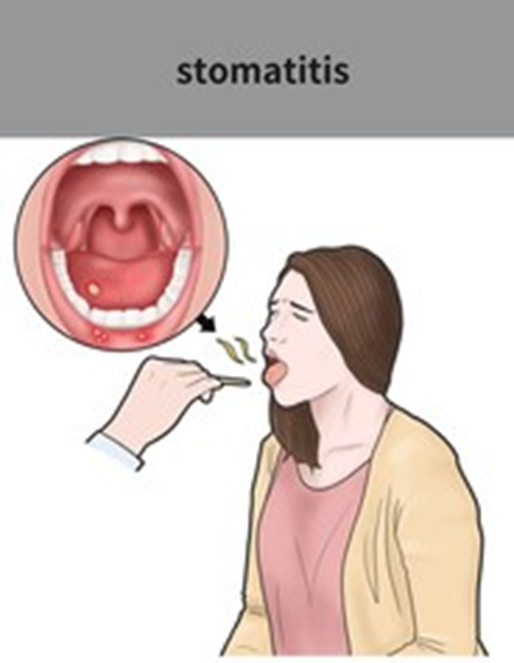
Choice a is not correct because providing an alcohol-based mouthwash is an action that the nurse should avoid when caring for a client who has stomatitis. Alcohol can dry and irritate the oral mucosa and worsen the condition.
Choice b is not correct because minimizing the use of gravies and sauces is not an action that the nurse should take to help manage stomatitis. Gravies and sauces can help moisten dry foods and make them easier to swallow for a client who has stomatitis.
Choice d is not correct because discouraging drinking with a straw is not an action that the nurse should take to help manage stomatitis. Drinking with a straw can help prevent contact between fluids and sore areas of the mouth and reduce pain for a client who has stomatitis.
Correct Answer is C
Explanation
Choice A reason: Eliminating egg whites from the diet is not necessary, as they are a good source of protein and do not contain any fat or cholesterol. The client should limit or avoid egg yolks, which are high in cholesterol and saturated fat.
Choice B reason: Using coconut oil when preparing food is not advisable, as it is a source of saturated fat that can raise blood cholesterol levels and increase the risk of atherosclerosis and heart disease. The client should use unsaturated fats, such as olive oil or canola oil, which can lower blood cholesterol levels and improve heart health.
Choice C reason: Eating fish three times a week is a good practice, as fish are rich in omega-3 fatty acids that can reduce inflammation, lower blood pressure, and prevent blood clots that can cause heart attacks or strokes. The client should choose oily fish, such as salmon, tuna, or mackerel, which have higher amounts of omega-3 fatty acids.
Choice D reason: Including 2 percent milk in the diet is not recommended, as it contains more fat and calories than skim or 1 percent milk. The client should choose low-fat or fat-free dairy products, such as yogurt, cheese, or milk, which can provide calcium and protein without excess fat.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today