A nurse is assessing a client who has fluid volume deficit. The nurse should expect which of the following findings?
Increased BUN
Increased urine ketones
Decreased urine specific gravity
Decreased Hgb
The Correct Answer is A
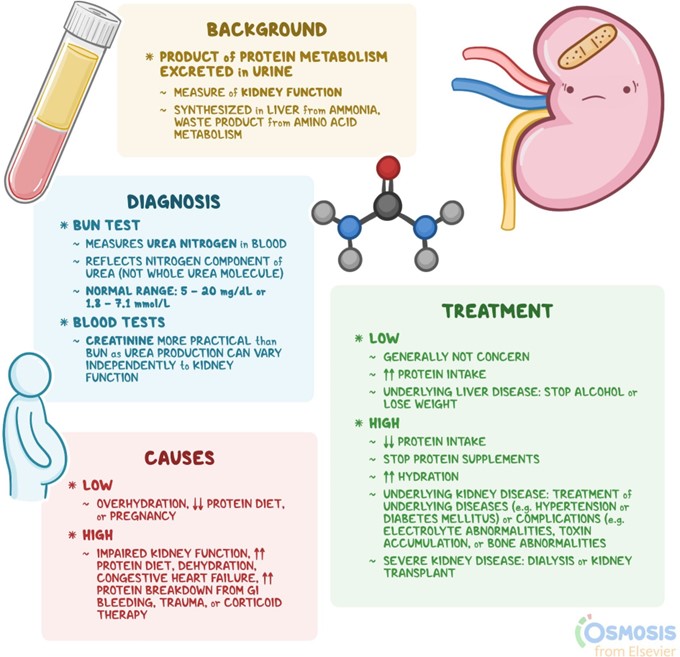
Choice A Reason: This is correct because BUN stands for blood urea nitrogen, which is a waste product of protein metabolism that is excreted by the kidneys. Increased BUN indicates fluid volume deficit, as the blood becomes more concentrated and the kidneys have less fluid to filter. A normal BUN level is 7 to 20 mg/dL. The nurse should monitor the client's fluid intake and output, weight, and serum electrolytes, and administer fluids as ordered.
Choice B Reason: This is incorrect because urine ketones are not related to fluid volume deficit, but to diabetic ketoacidosis, which is a complication of diabetes mellitus that occurs when the body breaks down fat for energy and produces ketones as a by-product. Increased urine ketones indicate diabetic ketoacidosis, which can cause
dehydration, acidosis, and coma. A normal urine ketone level is negative or trace. The nurse should monitor the client's blood glucose, pH, and bicarbonate levels, and administer insulin and fluids as ordered.
Choice C Reason: This is incorrect because urine specific gravity is a measure of the concentration of solutes in the urine. Decreased urine specific gravity indicates fluid volume excess, as the urine becomes more diluted and the kidneys excrete more fluid. A normal urine specific gravity range is 1.005 to 1.030. The nurse should monitor the client's fluid balance, vital signs, and edema, and administer diuretics as ordered.
Choice D Reason: This is incorrect because Hgb stands for hemoglobin, which is a protein in red blood cells that carries oxygen. Decreased Hgb indicates anemia, which is a condition that occurs when the blood has a low number of red blood cells or hemoglobin. Anemia can cause fatigue, weakness, and pallor. A normal Hgb level for adult males is 14 to 18 g/dL and for adult females is 12 to 16 g/dL. The nurse should monitor the client's oxygen saturation, iron level, and blood transfusion needs, and administer iron supplements or erythropoietin as ordered.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","B","D"]
Explanation
Choice A: Bicarbonate excess is a sign of metabolic alkalosis, because this condition occurs when the body has too much bicarbonate or loses too much acid. This can happen in patients who have excessive vomiting, gastric suctioning, diuretic therapy, or antacid intake.
Choice B: Lethargy is a sign of metabolic alkalosis, because this condition affects the central nervous system and causes decreased level of consciousness, confusion, and drowsiness. Lethargy can also result from hypoxemia, which is a condition that occurs when the blood oxygen level is too low. This can happen in patients with metabolic alkalosis who have respiratory compensation and hypoventilation.
Choice C: Kussmaul's respirations are not a sign of metabolic alkalosis, but rather of metabolic acidosis. This is a condition that occurs when the body produces too much acid or loses too much bicarbonate. This can happen in patients who have diabetic ketoacidosis, renal failure, or lactic acidosis. Kussmaul's respirations are deep, rapid, and labored breathing that help to eliminate excess carbon dioxide and acid from the blood.
Choice D: Circumoral paresthesia is a sign of metabolic alkalosis, because this condition causes hypocalcemia, which is a condition that occurs when the blood calcium level is too low. This can happen in patients with metabolic alkalosis who have increased binding of calcium to albumin due to alkaline pH. Circumoral paresthesia is a tingling sensation around the mouth that indicates neuromuscular irritability.
Choice E: Flushing is not a sign of metabolic alkalosis, but rather of hypercalcemia, which is a condition that occurs when the blood calcium level is too high. This can happen in patients who have hyperparathyroidism, malignancy, or excessive calcium intake. Flushing is a reddening of the skin that indicates vasodilation and increased blood flow.
Correct Answer is A
Explanation
- Choice A Reason: This is correct because the client who has gastroenteritis and is febrile is likely to lose fluid through vomiting, diarrhea, and sweating. These losses can lead to dehydration, hypotension, and electrolyte imbalances. The nurse should monitor the client's vital signs, fluid intake and output, and weight, and administer fluids and electrolytes as ordered.
- Choice B Reason: This is incorrect because the client who has leftsided heart failure and has a BNP level of 600 pg/ml is likely to have fluid volume excess, not deficit. BNP is a hormone that is released by the heart when it is stretched by increased blood volume. A high BNP level indicates that the heart is failing to pump effectively and that fluid is accumulating in the lungs and other tissues. The nurse should monitor the client's respiratory status, oxygen saturation, edema, and weight, and administer diuretics and other medications as ordered.
- Choice C Reason: This is incorrect because the client who has endstage renal failure and is scheduled for dialysis today is likely to have fluid volume excess, not deficit. Renal failure impairs the kidney's ability to excrete fluid and waste products, leading to fluid retention and azotemia. Dialysis is a procedure that removes excess fluid and toxins from the blood using an artificial membrane. The nurse should monitor the client's blood pressure, fluid intake and output, weight, and laboratory values, and prepare the client for dialysis as ordered.
- Choice D Reason: This is incorrect because the client who has been NPO since midnight for endoscopy is unlikely to have a significant fluid volume deficit, unless they have other risk factors or comorbidities. NPO means nothing by mouth, which is a common instruction before certain procedures or surgeries to prevent aspiration. Endoscopy is a procedure that uses a flexible tube with a camera to examine the digestive tract. The nurse should verify the client's NPO status, check their consent form, and administer preoperative medications as ordered.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today