A nurse is assessing a client who has post-traumatic stress disorder. Which of the following findings should the nurse expect? (Select all that apply.)
Blames others for own mistakes
Has difficulty concentrating on set tasks
Difficulty falling or staying asleep
Holds persistent negative belief about self
Talks excessively
Correct Answer : B,C,D
A. Blaming others for one's own mistakes is not typically associated with PTSD. Individuals with PTSD may have heightened irritability or anger, but this does not necessarily translate to blaming others.
B. Difficulty concentrating on tasks is a common symptom of PTSD as individuals may be easily distracted by intrusive thoughts related to their trauma.
C. Difficulty falling or staying asleep is another symptom often reported by individuals with PTSD, which can be attributed to hyperarousal and intrusive thoughts.
D. Holding persistent negative beliefs about oneself is indicative of the negative alterations in cognition and mood associated with PTSD.
E. Talking excessively is not a common finding in PTSD. While some individuals may speak more when anxious, it is not a diagnostic criterion for PTSD.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
A. Allowing the client to create their own meal schedule may exacerbate disordered eating patterns and is not recommended in the treatment of bulimia nervosa.
B. Allowing the client's family to bring food may enable or reinforce disordered eating behaviors and is not recommended in the treatment of bulimia nervosa.
C. Monitoring the client's bathroom trips is important to prevent purging behaviors, such as self- induced vomiting, which are characteristic of bulimia nervosa.
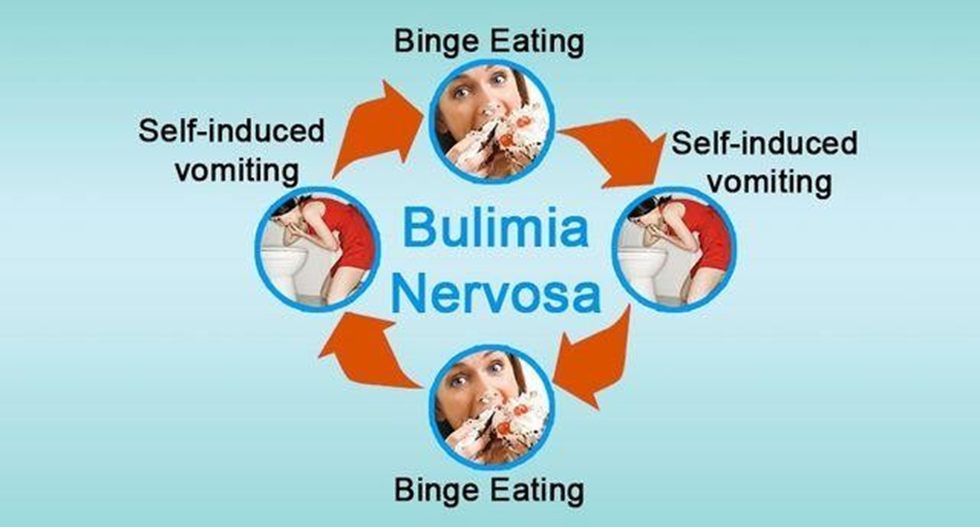
D. Encouraging the client to exercise frequently may exacerbate unhealthy behaviors and is not recommended as a primary intervention for bulimia nervosa.
Correct Answer is D
Explanation
A. Administering medications, such as atropine, requires nursing judgment and assessment of the client's condition, which should not be delegated to assistive personnel.
B. Witnessing the client's signature on the consent form ensures that the client provides informed consent for the procedure and requires nursing judgment.
C. Assessing the client's condition after the procedure involves monitoring vital signs, level of consciousness, and potential adverse reactions, which require nursing assessment and judgment.
D. Assisting the client to ambulate after the procedure is a task that can be safely delegated to assistive personnel, as long as the client's condition is stable and there are no contraindications to ambulation.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today