A nurse is assessing a newborn following a circumcision. Which of the following findings should the nurse identify as an indication that the newborn is experiencing pain?
Decreased heart rate
Chin quivering
Pinpoint pupils
Slowed respirations
The Correct Answer is B
A. Decreased heart rate: This is not typically an indication of pain in a newborn. Pain can often lead to an increased heart rate as the body responds to stress or discomfort.
B. Chin quivering: This is a common sign of pain in newborns. When infants experience pain, they may exhibit facial expressions such as quivering of the chin, furrowing of the brow, or grimacing.
C. Pinpoint pupils: Pinpoint pupils are not a typical sign of pain in a newborn. This may be associated with certain medications or conditions affecting the nervous system, but it is not a direct indicator of pain.
D. Slowed respirations: While pain can sometimes cause changes in respiratory patterns, slowed respirations alone may not be a reliable indicator of pain in a newborn. Other signs, such as facial expressions or crying, are often more indicative of pain.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
The correct answer is B. The client will experience a successful induction of labor.
A. The Bishop score is a pre-induction assessment that evaluates several factors, including cervical dilation, effacement, consistency, position, and fetal station. It is used to predict the likelihood of a successful induction of labor. A high Bishop score indicates favorable conditions for induction.
B. Correct. A higher Bishop score indicates a more favorable cervix for induction, and the chances of a successful induction of labor are increased.
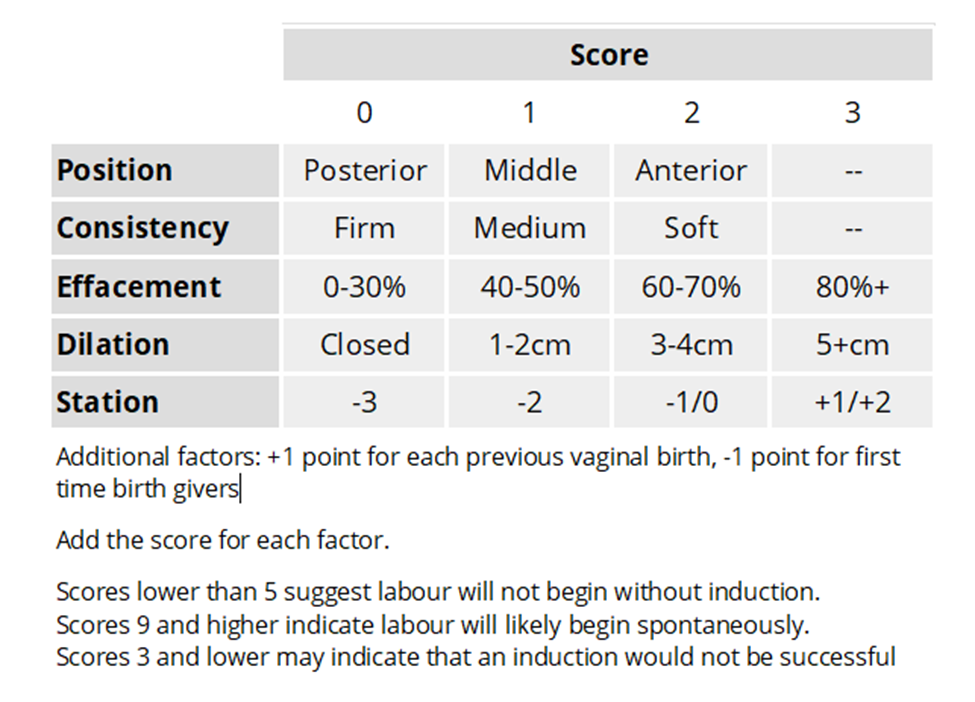
C. Lower back pain during labor is not specifically associated with the Bishop score. It can be a common complaint during labor, but it is not predicted by the Bishop score.
D. Dinoprostone is a prostaglandin used for cervical ripening. If the Bishop score indicates an unfavorable cervix, dinoprostone or other cervical ripening agents may be considered to prepare the cervix for induction.
Correct Answer is C
Explanation
Choice A Reason:
Left upper quadrant is incorrect. The left upper quadrant is less likely to be the area where the point of maximum intensity of the fetal heart is heard when the fetal position is left occipital anterior.
Choice B Reason:
Right upper quadrant is incorrect. The right upper quadrant is not the typical location for assessing fetal heart tones when the fetal position is left occipital anterior. The heart tones are generally heard more towards the left side.
Choice C Reason:
Left lower quadrant is correct. Placing the ultrasound transducer in the left lower quadrant is likely to provide the best detection of the fetal heart tones in the described fetal position.
Choice D Reason:
Right lower quadrant is incorrect. Similar to the right upper quadrant, the right lower quadrant is not the optimal location for assessing the fetal heart when the fetal position is left occipital anterior. The left side is typically where the point of maximum intensity is found.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today