A nurse is assisting in the admission process for a client who has a history of violent behavior. The client stands up and begins clenching her fists and arguing with the nurse. Which of the following actions is the priority?
Explore the truth of the client's statements.
Establish a therapeutic nurse-client relationship.
Set behavioral limits for the client
Show the client around the unit and introduce her to other clients.
The Correct Answer is C
The priority action in this situation is to set behavioral limits for the client. This is important for maintaining a safe environment for the client, other staff members, and other clients. By setting limits, the nurse establishes clear boundaries and expectations for behavior, helping to prevent the escalation of aggression or violence.
Let's examine why the other choices are incorrect:
A. Exploring the truth of the client's statements: While it is important to listen to and validate the client's concerns, in this particular situation, where the client is becoming agitated and confrontational, addressing the truth of their statements is not the priority. The immediate concern is ensuring safety and de-escalating the situation.
B. Establishing a therapeutic nurse-client relationship: Developing a therapeutic relationship is crucial for providing effective care, but it may not be the immediate priority when a client is displaying aggressive or violent behavior. Safety takes precedence in such situations, and setting behavioral limits is necessary before establishing a therapeutic relationship can effectively occur.
D. Showing the client around the unit and introducing her to other clients: This action is inappropriate during an agitated and confrontational episode. It is important to first
address the client's behavior and ensure the safety of all individuals involved before engaging in social activities or introductions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
This response reflects active listening and demonstrates empathy towards the client's feelings. It acknowledges the client's distress and encourages them to express their concerns and thoughts. By actively listening and showing genuine interest, the nurse can gather more information to assess the client's needs and determine the appropriate course of action.
Let's discuss why the other options are incorrect:
A. "Everything will be okay until morning. You can speak with your provider then." This response may dismiss or invalidate the client's current distress and fails to address their immediate concerns. It suggests waiting until morning without exploring the reasons behind the client's urgency.
C. "Go back to your room, and I'll try to get in touch with your provider in the morning." While the intention may be to offer assistance, this response does not address the client's emotional state or explore the reasons for their demand to see the provider. It may also not address the client's immediate needs and concerns.
D. "Why don't you wait until the morning? The provider will be available then." This response may come across as dismissive and may not acknowledge the client's current distress. It does not encourage the client to express their concerns or provide an opportunity for open communication.
Correct Answer is D
Explanation
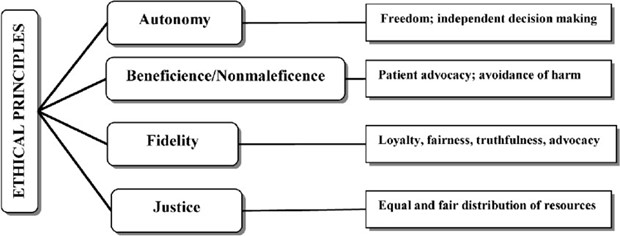
Autonomy is the ethical principle that upholds an individual's right to make decisions about their own care and treatment. Respecting autonomy means acknowledging and honoring a person's right to make choices based on their own values, beliefs, and preferences. By importing a client's wishes to refuse prescribed treatments, the nurse is recognizing and respecting the client's autonomy. This shows that the nurse values the client's right to make decisions about their own healthcare and supports their choice, even if it may differ from what the nurse may recommend.
Incorrect:
A. Spending extra time to calm an agitated client demonstrates the ethical principle of beneficence, which is the duty to promote the well-being and welfare of the client.
B. Ensuring that a client understands expectations for group participation relates to the ethical principle of fidelity, which involves maintaining trust and keeping promises to the client.
C. Describing the adverse effects of a client's medications is important for informed consent and promoting understanding, but it does not directly involve the client's autonomy unless it is accompanied by a discussion of the client's choices and preferences regarding medication.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today