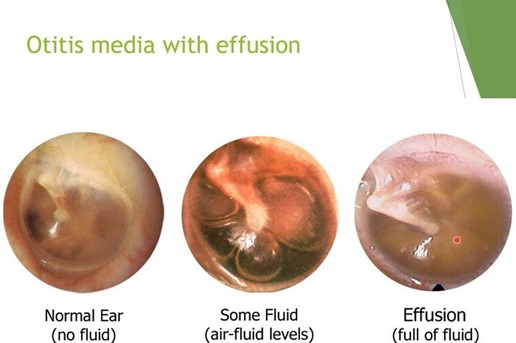
A nurse is caring for a child who has otitis media with effusion. The nurse should identify which of the following manifestations indicates a tympanic membrane rupture.
Popping sensation when swallowing
Green-blue discharge in the ear canal
Sudden pain relief
Increased temperature
The Correct Answer is C
Choice A: A popping sensation when swallowing is not a sign of a tympanic membrane rupture, as it is a normal phenomenon that occurs when the eustachian tube opens and closes to equalize the pressure between the middle ear and the atmosphere. A popping sensation when swallowing may be associated with otitis media with effusion, which is a condition that causes fluid accumulation behind the eardrum, but it does not indicate a rupture.
Choice B: Green-blue discharge could be indicative of infection but is not as directly related to the rupture event as the sudden pain relief is.
Choice C: The correct answer is sudden relief of pain. This is because the rupture of the tympanic membrane releases the pressure and fluid that has built up in the middle ear, leading to an immediate decrease in pain.
Choice D: An increased temperature is not a sign of a tympanic membrane rupture, as it is a nonspecific symptom that may indicate various conditions, such as inflammation, infection, or fever. An increased temperature may be associated with otitis media with effusion, which is a condition that causes fluid accumulation behind the eardrum, but it does not indicate a rupture.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A: This statement does not indicate a need for further teaching, as it is correct that insulin can be injected anywhere there is adipose tissue. Adipose tissue is the layer of fat under the skin that can absorb insulin and prevent damage to muscles or organs. The common sites for insulin injection are the abdomen, thighs, buttocks, or upper arms.
Choice B: This statement does not indicate a need for further teaching, as it is correct that the child should rotate sites after 5 injections in one area. Rotating sites can prevent lipodystrophy, which is a condition that causes abnormal changes in fat tissue due to repeated injections. Lipodystrophy can affect the appearance and absorption of insulin in the affected area.
Choice C: This statement indicates a need for further teaching, as it is incorrect that the child should aspirate before injecting the insulin. Aspiration is the process of pulling back on the plunger of the syringe to check for blood before injecting the medication. Aspiration is not recommended for insulin injection, as it can cause pain, bruising, or leakage of insulin from the injection site.
Choice D: This statement does not indicate a need for further teaching, as it is correct that insulin should be injected at a 90-degree angle. Injecting insulin at a 90-degree angle can ensure that the medication reaches the adipose tissue and prevents skin irritation or muscle damage. The only exception is if the child has very thin skin or uses very short needles, in which case they may inject at a 45-degree angle.

Correct Answer is B
Explanation
Choice A: A 3-year-old child is not developmentally ready to descend stairs by placing both feet on each step and holding on to the railing. A 3-year-old child can walk up stairs alternating feet with one hand held by an adult or on the railing. A 3-year-old child can also walk down stairs placing both feet on each step with one hand held by an adult.
Choice B: A 4-year-old child is developmentally able to descend stairs by placing both feet on each step and holding on to the railing. A 4-year-old child can also walk up stairs alternating feet without assistance.
Choice C: A 5-year-old child is developmentally more advanced than descending stairs by placing both feet on each step and holding on to the railing. A 5-year-old child can walk up and down stairs alternating feet without assistance.
Choice D: A 6-year-old child is developmentally more advanced than descending stairs by placing both feet on each step and holding on to the railing. A 6-year-old child can walk up and down stairs alternating feet without assistance and can also hop and skip on one foot.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today