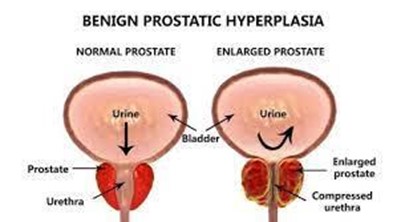
A nurse is caring for a client who has benign prostatic hyperplasia (BPH). Which of the following findings should the nurse expect?
Painful urination
Decreased urinary stream
Critically elevated prostate-specific antigen (PSA) level
Urge incontinence
The Correct Answer is B
Choice A Reason: Painful urination is not a common finding in BPH, but it may indicate a urinary tract infection or bladder stones.
Choice B Reason: Decreased urinary stream is a common finding in BPH, as the enlarged prostate compresses the urethra and obstructs the flow of urine.
Choice C Reason: Critically elevated PSA level is not a common finding in BPH, but it may indicate prostate cancer or prostatitis.
Choice D Reason: Urge incontinence is not a common finding in BPH, but it may indicate an overactive bladder or neurogenic bladder.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: If I feel nervous or have tremors, I should not only take half the dose, but I should contact my healthcare provider, as these may indicate signs of overdose or hyperthyroidism.
Choice B Reason: I cannot expect diarrhea, insomnia, and excessive sweating, but these are possible side effects of overdose or hyperthyroidism.
Choice C Reason: I need to call my healthcare provider if my heart rate becomes fast, as this may indicate a serious adverse reaction or overdose of levothyroxine sodium.
Choice D Reason: I should not take the medication in the evening, but in the morning on an empty stomach at least 30 minutes before breakfast, as this ensures better absorption and prevents insomnia.
Correct Answer is C
Explanation
Choice A Reason: Encouraging deep-breathing exercises is not the most appropriate nursing intervention, as it may not reduce fatigue and may increase respiratory effort.
Choice B Reason: Providing a relaxing warm bath is not the most appropriate nursing intervention, as it may worsen fatigue and increase the risk of heat intolerance and dehydration.
Choice C Reason: Scheduling periods of rest in between activities is the most appropriate nursing intervention, as it helps to conserve energy, prevent exhaustion, and promote recovery.
Choice D Reason: Administering multivitamins is not the most appropriate nursing intervention, as it may not improve fatigue and may cause adverse effects or interactions with other medications.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today