A client has been diagnosed with hypothyroidism. What information should the nurse obtain when conducting a focused assessment? Select all that apply.
Weight gain
Constipation
Rapid pulse
Decreased energy
Hypertension
Correct Answer : A,B,D
Choice A Reason: Weight gain is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the metabolism to slow down and the body to store more fat.
Choice B Reason: Constipation is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the gastrointestinal motility to decrease and the stools to become hard and dry.
Choice C Reason: Rapid pulse is not a common finding in hypothyroidism, but it may indicate other conditions such as hyperthyroidism or anxiety.
Choice D Reason: Decreased energy is a common finding in hypothyroidism, as the decreased thyroid hormone level causes the body to feel tired and sluggish.
Choice E Reason: Hypertension is not a common finding in hypothyroidism, but it may indicate other conditions such as renal disease or cardiovascular disease.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A Reason: Lantus is not a type of insulin that can treat this client, as it is a long-acting insulin that has no peak effect and lasts for 24 hours.
Choice B Reason: NPH is not a type of insulin that can treat this client, as it is an intermediate-acting insulin that peaks in 6 to 8 hours and lasts for 12 to 18 hours.
Choice C Reason: Regular is a type of insulin that can treat this client, as it is a short-acting insulin that peaks in 2 to 4 hours and lasts for 6 to 8 hours. It can be used to correct high blood glucose levels and treat diabetic ketoacidosis (DKA), which is indicated by confusion, flushing, and acetone breath.
Choice D Reason: Lispro is not a type of insulin that can treat this client, as it is a rapid-acting insulin that peaks in 30 minutes and lasts for 3 to 5 hours. It can be used to cover meals or snacks but not to treat DKA.
Correct Answer is D
Explanation
Choice A Reason: Side lying on the affected eye is not the correct position for the client after cataract surgery, as it may increase intraocular pressure and cause bleeding or damage to the surgical site.
Choice B Reason: Supine is not the correct position for the client after cataract surgery, as it may cause fluid accumulation and swelling in the eye.
Choice C Reason: Prone is not the correct position for the client after cataract surgery, as it may cause pressure and friction on the eye.
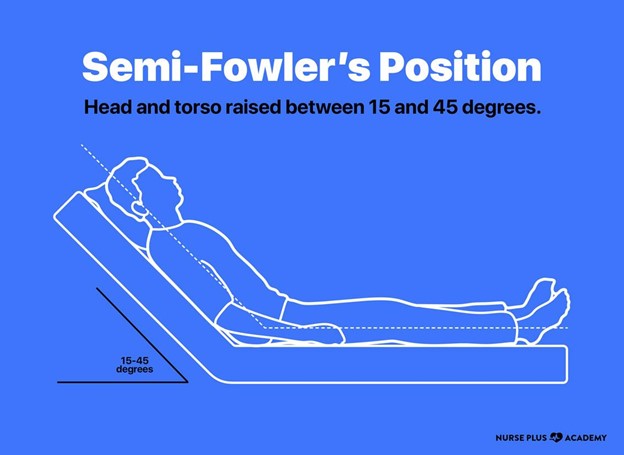
Choice D Reason: Semi Fowler's is the correct position for the client after cataract surgery, as it helps to reduce intraocular pressure and promote drainage and healing of the eye.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today