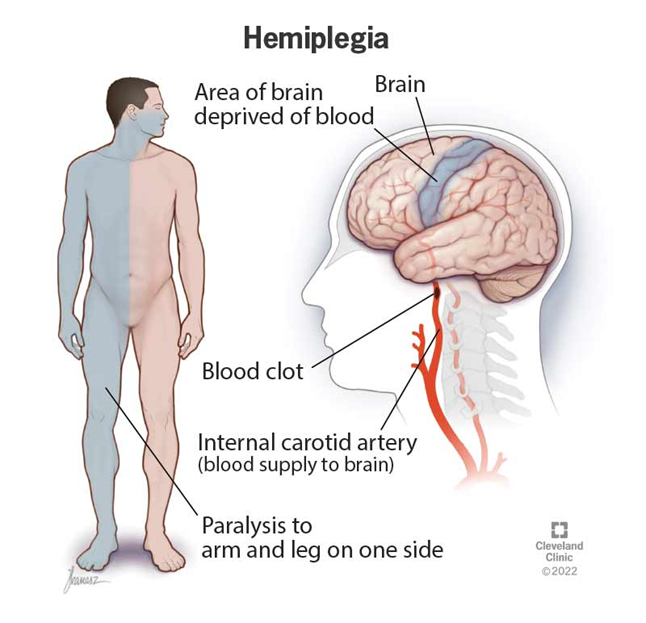
A nurse is caring for a client who has right-sided hemiplegia following a recent stroke. Which of the following questions should the nurse ask to determine the client's ability to cope?
"Why do you think this has happened?"
"Are you okay with not being able to do some things you used to do?"
"Is anyone available to assist you with your hygiene?"
"How has this impacted your life?"
The Correct Answer is D
Choice A reason:
Asking "Why do you think this has happened?" may not be the most supportive approach. This question can lead to feelings of guilt or frustration, as the client might not have an answer and could feel blamed for their condition. It is more beneficial to focus on the client's current feelings and coping mechanisms.
Choice B reason:
Asking "Are you okay with not being able to do some things you used to do?" can be perceived as insensitive. It highlights the client's limitations rather than focusing on their strengths and coping strategies. This question might make the client feel more helpless and discouraged.
Choice C reason:
Asking "Is anyone available to assist you with your hygiene?" is important for assessing the client's support system and daily needs, but it does not directly address their emotional coping. While practical support is crucial, understanding the client's emotional and psychological state is equally important.
Choice D reason:
Asking "How has this impacted your life?" is an open-ended question that allows the client to express their feelings and experiences. It helps the nurse understand the client's perspective and coping mechanisms. This question encourages the client to share their emotional journey and can provide valuable insights into their mental and emotional well-being.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Choice A reason:
Asking the client's family to encourage the client to receive ECT may be a supportive measure, but it should not be the first action taken. The client's autonomy and right to refuse treatment must be respected, even if they are involuntarily committed. Family members can be involved in the discussion, but the client's decision should be paramount.
Choice B reason:
Telling the client they cannot refuse treatment because they were involuntarily committed is incorrect. Involuntary commitment does not automatically override a client's right to refuse treatment. Clients have the right to be informed about their treatment and to refuse it unless specific legal criteria are met.
Choice C reason:
Documenting the client's refusal of the treatment in the medical record is the correct action. It is essential to record the client's decision and the discussion surrounding it. This documentation ensures that the client's rights are respected and provides a legal record of the interaction.
Choice D reason:
Informing the client that ECT does not require client consent is incorrect and unethical. Consent is a fundamental patient right, and all clients, including those involuntarily committed, have the right to be informed about their treatment options and to give or withhold consent unless they are legally deemed incompetent to make such decisions.
Correct Answer is A
Explanation
Choice A reason:
Suppression is a conscious defense mechanism where an individual intentionally avoids thinking about disturbing thoughts or feelings. In this case, the client is choosing to delay addressing the reality of their diagnosis until after a significant family event. This can be seen as a temporary coping strategy to manage overwhelming emotions, but it may become maladaptive if overused or if it prevents the client from seeking necessary treatment and support.
Choice B reason:
Compensation involves overachieving in one area to make up for deficiencies in another. The client's statement does not suggest that they are trying to compensate for their illness by excelling in other areas of life; rather, they are postponing the emotional processing of their diagnosis.
Choice C reason:
Regression is a return to earlier stages of development and coping strategies, often under stress. The client's statement does not indicate a regression to more childlike behaviors or earlier developmental stages.
Choice D reason:
Sublimation is a way of channeling unacceptable impulses into socially acceptable actions. The client's statement does not reflect the use of sublimation, as they are not redirecting their feelings about the diagnosis into a different, more acceptable outlet.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today