A nurse is caring for a client who has urinary leakage due to nerve damage following a spinal cord injury. The nurse should identify that the client is experiencing which of the following types of urinary incontinence?
Overflow incontinence
Urge incontinence
Stress incontinence
Reflex incontinence
The Correct Answer is D
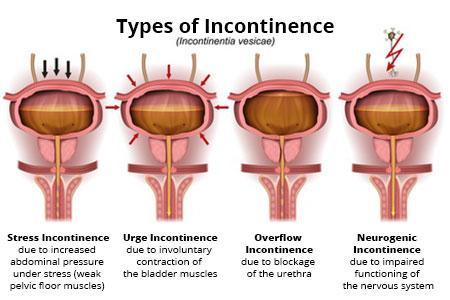
Choice A reason: Overflow incontinence is not the type of urinary incontinence that the client is experiencing. Overflow incontinence occurs when the bladder is overfilled and cannot empty properly, causing frequent or constant dribbling of urine. It can be caused by a blockage in the urinary tract, such as an enlarged prostate or a kidney stone, or by a weak bladder muscle that cannot contract enough to empty the bladder.
Choice B reason: Urge incontinence is not the type of urinary incontinence that the client is experiencing. Urge incontinence occurs when the bladder muscle contracts involuntarily and causes a sudden and strong urge to urinate, followed by an involuntary loss of urine. It can be caused by an infection, a neurological disorder, or an overactive bladder.
Choice C reason: Stress incontinence is not the type of urinary incontinence that the client is experiencing. Stress incontinence occurs when the pelvic floor muscles or the urethral sphincter are weakened or damaged and cannot hold urine in the bladder when there is increased abdominal pressure, such as from coughing, sneezing, laughing, or exercising. It can be caused by pregnancy, childbirth, menopause, or surgery.
Choice D reason: Reflex incontinence is the type of urinary incontinence that the client is experiencing. Reflex incontinence occurs when the bladder muscle contracts without the sensation or control of the person, causing urine to leak without warning or awareness. It can be caused by nerve damage that affects the communication between the bladder and the brain, such as from a spinal cord injury, a stroke, or multiple sclerosis..
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A reason: Administering the medication 2 hr before exercise is a correct instruction for the parent of a child who has asthma and a prescription for montelukast granules. Montelukast is a leukotriene modifier that helps to prevent asthma attacks and exercise induced bronchoconstriction. It is taken once a day in oral form and may cause side effects such as stomach pain, diarrhea, or mood changes. For children who have exercise induced asthma, an additional dose of montelukast may be taken 2 hr before exercise.
Choice B reason: Giving the medication at the onset of wheezing is not a correct instruction for the parent of a child who has asthma and a prescription for montelukast granules. Montelukast is not a fast acting rescue medicine for asthma attacks and needs to be taken daily. It does not work quickly enough to relieve the symptoms of an acute asthma attack, such as wheezing, coughing, or shortness of breath. For an asthma attack, the child should use a short acting beta agonist inhaler, such as albuterol, as prescribed by the provider.
Choice C reason: Administering the granules mixed with 20 oz of water is not a correct instruction for the parent of a child who has asthma and a prescription for montelukast granules. Montelukast granules come in a sachet with 4 mg of granules inside (one dose). They can be placed directly on the child's tongue or mixed with a spoonful of cold or room temperature soft food, such as applesauce, mashed carrots, rice, or ice cream. They can also be mixed with 1 teaspoonful (5 mL) of cold or room temperature baby formula or breast milk. They should not be mixed with any other liquid drink other than baby formula or breast milk. The mixture should be taken within 15 minutes after opening the packet.
Choice D reason: Giving the medication in the morning daily is not a correct instruction for the parent of a child who has asthma and a prescription for montelukast granules. Montelukast works best when taken in the evening, as it can improve the symptoms of asthma and allergic rhinitis that occur at night or early in the morning. Taking it at the same time every day can also help to maintain a steady level of the drug in the body and prevent missed doses.
Correct Answer is C
Explanation
Choice A reason: Decrease respiratory secretions. This answer is incorrect because pancuronium does not have any effect on the production or clearance of respiratory secretions. This medication is not used to treat the pulmonary edema and inflammation that occur in ARDS.
Choice B reason: Induce sedation. This answer is incorrect because pancuronium does not have any sedative or analgesic properties. This medication does not affect the level of consciousness or pain perception of the client. A client who receives pancuronium should also receive adequate sedation and analgesia to prevent anxiety and discomfort.
Choice C reason: Suppress respiratory effort. This answer is correct because pancuronium is a neuromuscular blocker that inhibits the transmission of nerve impulses to the muscles, causing paralysis and relaxation. This medication is used to suppress the respiratory effort of the client and allow the mechanical ventilator to control the breathing.
Choice D reason: Decrease chest wall compliance. This answer is incorrect because pancuronium does not have any effect on the elasticity or stiffness of the chest wall. This medication is not used to treat the reduced lung compliance and increased airway resistance that occur in ARDS.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today