A nurse is caring for a client who is to have his chest tube removed. Which of the following actions should the nurse take?
Cover the insertion site with a hydrocolloid dressing.
Provide pain medication immediately after removal.
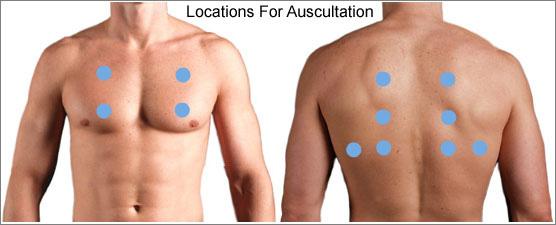
Auscultate the lungs after removal.
Delegate removal of the chest tube to an assistive personnel (AP).
The Correct Answer is C
Choice A reason: This is an incorrect action, because covering the insertion site with a hydrocolloid dressing can prevent air from escaping and cause a subcutaneous emphysema, which is a complication of chest tube removal. The insertion site should be covered with a sterile gauze dressing and taped on three sides.
Choice B reason: This is an important action, but not the first one. The nurse should provide pain medication before removal, not immediately after, to reduce the discomfort and anxiety of the client.
Choice C reason: This is the correct action, because auscultating the lungs after removal can help assess the respiratory status and detect any signs of pneumothorax, such as diminished or absent breath sounds.
Choice D reason: This is an incorrect action, because delegating removal of the chest tube to an AP is beyond the scope of practice and can cause harm to the client. The removal of the chest tube should be performed by the nurse or the provider.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
Choice A reason: This is an incorrect action, because elevating the residual limb on a soft pillow can cause contractures and impair the blood flow to the stump. The residual limb should be elevated only for the first 24 hr after surgery, and then positioned flat on the bed.
Choice B reason: This is the correct action, because assisting the client to a prone position every 4 hr can prevent hip flexion contractures and promote the range of motion of the hip joint. The client should lie prone for 20 to 30 minutes at a time, with the residual limb extended.
Choice C reason: This is an incorrect action, because reapplying a bandage to the residual limb every 12 hr can increase the risk of infection and delay the healing of the wound. The bandage should be changed only when it is soiled or loose, and under sterile technique.
Choice D reason: This is an incorrect action, because applying dressings to the site in a proximal-to-distal direction can cause edema and impair the circulation to
Correct Answer is C
Explanation
Choice A reason: Irrigating the catheter with sterile water is an incorrect action, because the catheter should be irrigated with sterile normal saline (0.9% sodium chloride) to prevent hemolysis of the red blood cells.
Choice B reason: Clamping the drainage catheter during ambulation is an incorrect action, because the catheter should be kept patent and unclamped at all times to prevent obstruction and infection.
Choice C reason: Reporting viscous drainage with clots to the provider is a correct action, because it indicates that the irrigation is not effective and the client may need manual irrigation or surgical intervention.
Choice D reason: Removing the catheter if the client feels a strong urge to urinate is an incorrect action, because the catheter should be left in place until the provider orders its removal. The client may feel a sensation of bladder fullness or spasms due to the irrigation fluid, which can be relieved by medication or adjustment of the flow rate.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today