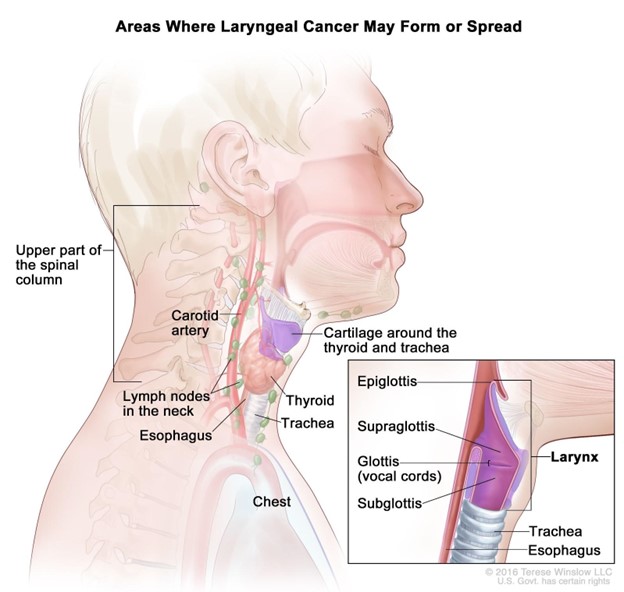
A nurse is collecting data from a client diagnosed with laryngeal cancer who is postoperative following a laryngectomy. Which of the following is a clinical manifestation of a hemorrhage?
Increased pain
Continuous swallowing
Poor fluid intake
Drooling
The Correct Answer is B
Choice A Reason: Increased pain is not a specific sign of hemorrhage, but it may indicate inflammation, infection, or nerve damage.
Choice B Reason: Continuous swallowing is a sign of hemorrhage, as it indicates that blood is accumulating in the throat or esophagus and stimulating the swallowing reflex.
Choice C Reason: Poor fluid intake is not a sign of hemorrhage, but it may indicate difficulty swallowing, nausea, or dehydration.
Choice D Reason: Drooling is not a sign of hemorrhage, but it may indicate impaired oral control, salivary gland damage, or infection.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is B
Explanation
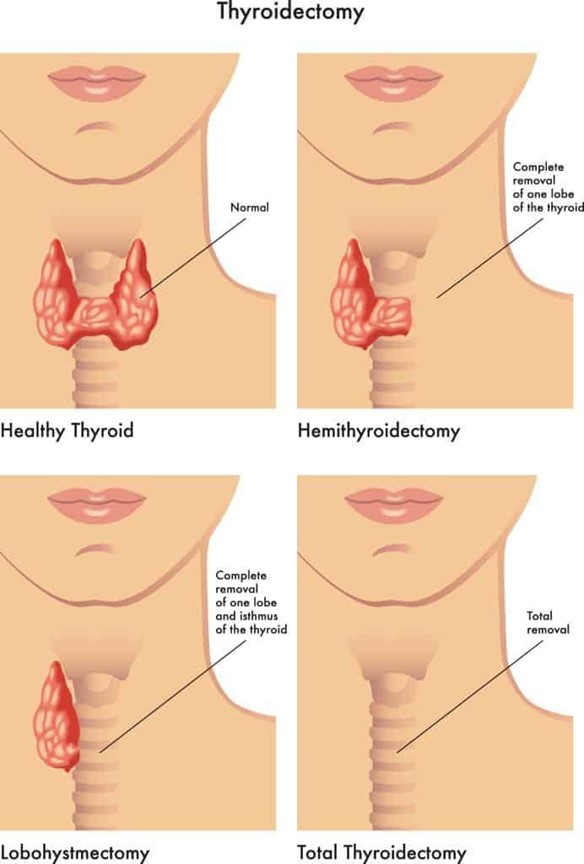
Choice A Reason: Encouraging the client to cough and deep breathe every two hours, with her neck in a flexed position, is not a priority for a client after a total thyroidectomy, as it may increase the risk of bleeding or damage to the surgical site.
Choice B Reason: Maintaining the client in a Fowler's position, with head neutral supported by pillows, is a priority for a client after a total thyroidectomy, as it helps to reduce swelling and edema, prevent airway obstruction, and promote venous drainage.
Choice C Reason: Maintaining the client in a supine position, with sandbags placed on either side of her head and neck, is not a priority for a client after a total thyroidectomy, as it may impair breathing and circulation, increase pressure on the surgical site, and cause neck stiffness.
Choice D Reason: Encouraging the client to turn head side to side, to promote drainage of oral secretions, is not a priority for a client after a total thyroidectomy, as it may cause pain and discomfort, disrupt the sutures or drains, and increase the risk of infection.
Correct Answer is D
Explanation
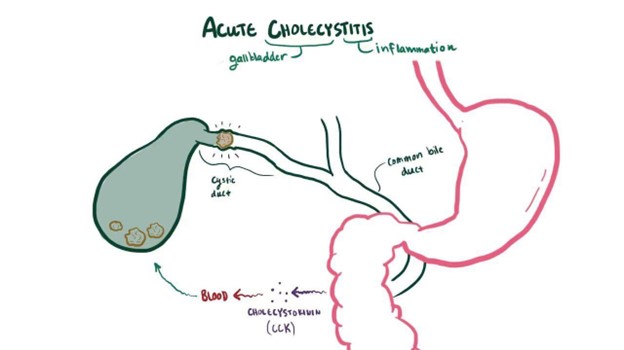
Choice A Reason: Ice cream is not a good food choice for a client who has cholecystitis, as it is high in fat and may trigger gallbladder pain or inflammation.
Choice B Reason: Blueberry muffin is not a good food choice for a client who has cholecystitis, as it may contain butter, oil, or eggs that are high in fat and may aggravate gallbladder symptoms.
Choice C Reason: Macaroni and cheese is not a good food choice for a client who has cholecystitis, as it is high in fat and cholesterol and may cause gallstone formation or obstruction.
Choice D Reason: Roast turkey is a good food choice for a client who has cholecystitis, as it is low in fat and high in protein and may help to prevent gallbladder attacks.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today