A nurse is collecting data from a client who has been admitted with suspected appendicitis. Which of the following findings is the nurse's priority to report to the provider?
Temperature 37.8° C (100° F)
Loss of appetite
WBC count 15,000/mm³
Rigid, board-like abdomen
The Correct Answer is D
Choice A reason: This is not a priority finding to report to the provider because temperature 37.8° C (100° F) indicates a mild fever that can be caused by inflammation or infection of the appendix or other organs. The nurse should monitor the client's temperature and administer antipyretics as prescribed.
Choice B reason: This is not a priority finding to report to the provider because loss of appetite is a common symptom of appendicitis that can result from nausea, vomiting, or pain. The nurse should encourage oral fluid intake and provide clear liquids or bland foods as tolerated.
Choice C reason: This is not a priority finding to report to the provider because WBC count 15,000/mm³ indicates leukocytosis or elevated white blood cell count that can be caused by inflammation or infection of the appendix or other organs. The nurse should monitor the client's laboratory values and administer antibiotics as prescribed.
Choice D reason: This is a priority finding to report to the provider because rigid, board-like abdomen indicates peritonitis or inflammation of the peritoneum that can be caused by rupture or perforation of the appendix or other organs. This is a medical emergency that requires immediate surgical intervention and aggressive fluid and antibiotic therapy. The nurse should assess the client's abdominal pain, distension, and guarding and notify the provider immediately.

Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
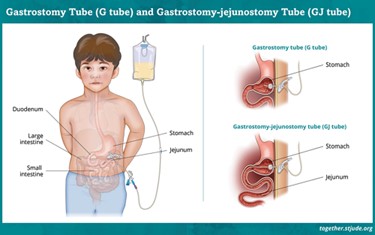
Choice A reason: Typically, the tube is flushed with about 30 mL of water before and after feedings to ensure patency and prevent clogging, not 90 mL.
Choice B reason: This is not an appropriate action because administering the feeding solution at a cold temperature can cause abdominal cramps, nausea, or vomiting. The nurse should warm the feeding solution to room temperature before administering it.
Choice C reason: Elevating the head of the bed helps prevent aspiration and promotes proper digestion by using gravity to keep the feeding solution in the stomach or jejunum.
Choice D reason: This is not an appropriate action because rotating the jejunostomy tube once per day can cause irritation or displacement of the tube. The nurse should secure the tube in place and check its position before each feeding.
Correct Answer is C
Explanation
Choice A reason: This is not an appropriate action because keeping the lights dimmed can increase the risk of falls, confusion, or agitation in the client who has Alzheimer's disease. The nurse should provide adequate lighting and reduce glare and shadows in the client's room and environment.
Choice B reason: This is not an appropriate action because alternating the client's daily routine can cause stress, anxiety, or frustration in the client who has Alzheimer's disease. The nurse should maintain a consistent and structured routine and schedule for the client and provide cues and reminders as needed.
Choice C reason: This is an appropriate action because participating in reminiscence therapy with the client can enhance their cognitive function, mood, and self-esteem by stimulating their long-term memory and encouraging them to share their past experiences, feelings, and values. The nurse should use photos, music, or objects that are meaningful to the client and listen actively and respectfully.
Choice D reason: This is not an appropriate action because raising the four side rails on the client's bed can be considered a form of restraint that can harm or injure the client who has Alzheimer's disease. The nurse should use alternative measures to ensure the client's safety and comfort, such as lowering the bed, using a bed alarm, or providing frequent supervision.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today