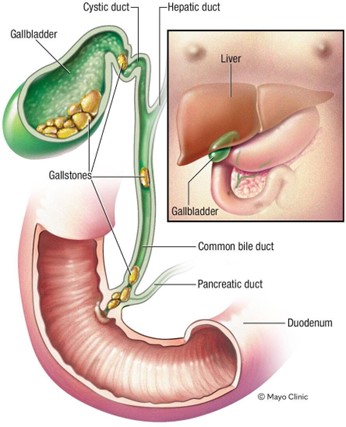
A nurse is collecting data from a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Which of the following findings is expected for this condition?
Faty stools
Ecchymosis of the extremities
Straw-colored urine
Tenderness in the left upper abdomen
The Correct Answer is A
Choice A: Faty stools. This is a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis, which is the presence of gallstones in the gallbladder or bile ducts. The common bile duct carries bile from the liver and gallbladder to the duodenum, where it helps digest fats. If the common bile duct is obstructed by a gallstone, bile cannot reach the duodenum and fats cannot be properly absorbed. This results in fatty stools, which are also known as steatorrhea. Fatty stools are pale, bulky, greasy, and foul-smelling.
Choice B: Ecchymosis of the extremities. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Ecchymosis of the extremities is a sign of bleeding under the skin, which can be caused by trauma, coagulation disorders, or medications. It is not related to bile duct obstruction or gallstones.
Choice C: Straw-colored urine. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Straw-coloured urine is a normal colour of urine, which indicates adequate hydration and kidney function. It is not affected by bile duct obstruction or gallstones.
Choice D: Tenderness in the left upper abdomen. This is not a finding that is expected for a client who has obstruction and inflammation of the common bile duct due to cholelithiasis. Tenderness in the left upper abdomen is a sign of splenomegaly, which is an enlargement of the spleen due to infection, inflammation, or cancer. It is not related to bile duct obstruction or gallstones.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
Choice A: “Monitor blood glucose levels every 4 hours.” This is the priority action for the nurse to recommend to the client because it will help them detect and prevent hyperglycemia or hypoglycemia, which can lead to serious complications such as diabetic ketoacidosis or cerebral edema.
Choice B: “Consume 15 grams of carbohydrates every 1 to 2 hours.” This is an important action for the nurse to recommend to the client, but not the priority. The client should consume carbohydrates to prevent hypoglycemia, especially if they have nausea, vomiting, or diarrhea, but this should be done after monitoring their blood glucose levels.
Choice C: “Drink 8 ounces of fluid every hour while awake.” This is a necessary action for the nurse to recommend to the client, but not the priority. The client should drink fluids to prevent dehydration and electrolyte imbalance, which can worsen hyperglycemia, but this should be done after monitoring their blood glucose levels.
Choice D: “Take the usual dosage of insulin.” This is a required action for the nurse to recommend to the client, but not the priority. The client should take their insulin as prescribed to control their blood glucose levels, but this should be done after monitoring their blood glucose levels and adjusting the dosage if needed.
Correct Answer is A
Explanation
Choice A: Potassium 2.5 mEq/L. This is the priority data collection finding that the nurse should identify according to the ABCDE principle, which prioritizes interventions based on airway, breathing, circulation, disability, and exposure. The nurse should identify potassium 2.5 mEq/L as the priority because it indicates hypokalemia, which is a low level of potassium in the blood. Potassium is an electrolyte that regulates the electrical activity of the heart and muscles. Hypokalemia can cause cardiac arrhythmias, muscle weakness, and paralysis, which can be life-threatening.
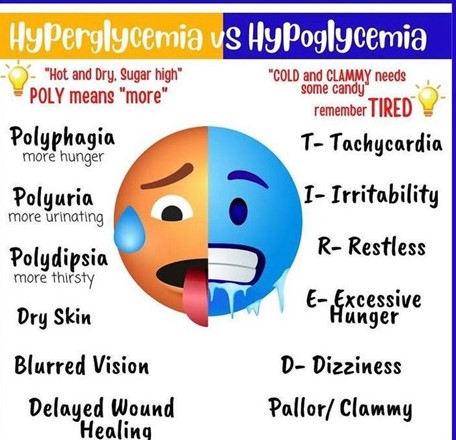
Choice B: Blood glucose 150 mg/dL. This is not the priority data collection finding that the nurse should identify for a client who has acute gastroenteritis. Blood glucose 150 mg/dL indicates hyperglycemia, which is a high level of glucose in the blood. Hyperglycemia can be caused by dehydration, stress, infection, or medication side effects.
Hyperglycemia can cause symptoms such as polyuria, polydipsia, polyphagia, and fatigue. It can also lead to complications such as diabetic ketoacidosis or hyperosmolar hyperglycemic state, which are serious but not as urgent as hypokalemia.
Choice C: Urine specific gravity 1.035. This is not the priority data collection finding that the nurse should identify for a client who has acute gastroenteritis. Urine specific gravity 1.035 indicates concentrated urine, which can be caused by dehydration or fluid loss. Dehydration can result from vomiting and diarrhea, which are common symptoms of acute gastroenteritis. Dehydration can cause symptoms such as dry mucous membranes, tachycardia, hypotension, and oliguria. It can also lead to complications such as shock or kidney failure, which are serious but not as urgent as hypokalemia.
Choice D: Weight loss of 3% of total body weight. This is not the priority data collection finding that the nurse should identify for a client who has acute gastroenteritis. Weight loss of 3% of total body weight indicates mild to moderate dehydration, which can be caused by fluid loss from vomiting and diarrhea. Weight loss can also reflect loss of muscle mass or fat tissue due to malnutrition or inflammation. Weight loss can affect the client’s nutritional status and immune function, but it is not as urgent as hypokalemia.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today