A nurse is collecting data on a client who has a stage 2 pressure injury. Which of the following findings should the nurse expect?
Intact skin with localized erythema.
Full thickness skin loss with visible bone
Full thickness skin loss with visible adipose tissue.
Partial-thickness skin loss with red tissue in wound bed.
The Correct Answer is D
A. Intact skin with localized erythema:
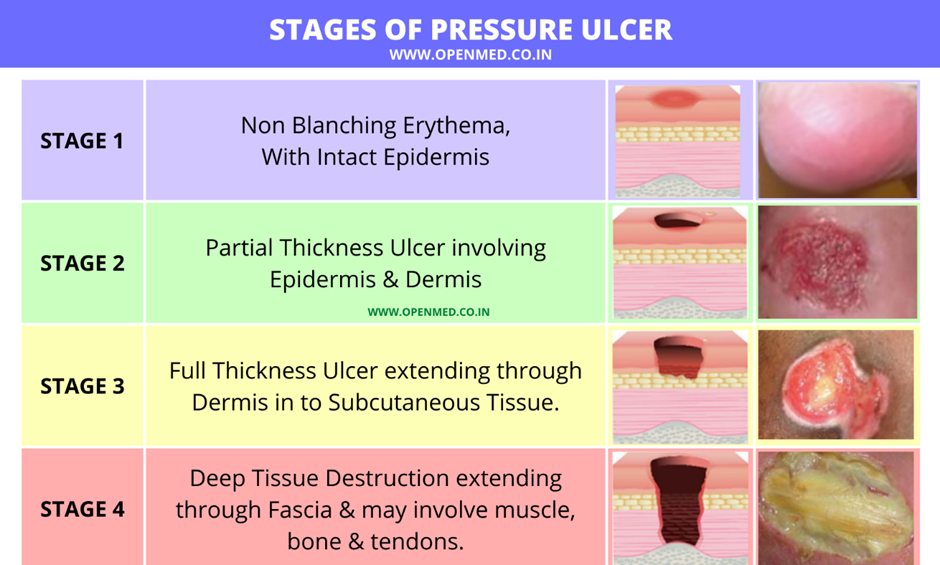
Explanation: This description is more consistent with a stage 1 pressure injury, where there is non-blanchable erythema.
B. Full thickness skin loss with visible bone:
Explanation: This description is more consistent with a stage 4 pressure injury, which involves extensive tissue loss, including exposure of bone.
C. Full thickness skin loss with visible adipose tissue:
Explanation: This finding is characteristic of a stage 3 pressure injury, where the loss of tissue extends down to the subcutaneous layer.
D. Partial-thickness skin loss with red tissue in the wound bed:
Explanation: This description is consistent with a stage 2 pressure injury, where there is partial-thickness skin loss involving the epidermis and possibly the dermis, forming a shallow open ulcer with a red-pink wound bed.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
No explanation
Correct Answer is A
Explanation
A.Adequate protein intake is essential for skin repair and maintaining skin integrity. Protein helps in the healing process, supports the immune system, and strengthens the skin, making it more resistant to breakdown. This is a crucial intervention for preventing pressure ulcers and promoting overall skin health in older adults.
B.Massaging bony prominences is not recommended as it can cause friction and damage to already vulnerable skin, increasing the risk of skin breakdown rather than preventing it. Gentle repositioning is preferred to relieve pressure.
C.Clients at risk for skin breakdown should typically be repositioned at least every 2 hours, not every 3 hours, to relieve pressure and reduce the risk of developing pressure ulcers. Therefore, this option is not ideal as stated.
D.While keeping the skin dry is important, cornstarch is not recommended because it can cake and cause friction, which may lead to skin breakdown. Using moisture-wicking products or barrier creams is more appropriate for maintaining skin dryness and integrity.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today