A nurse is counseling a client who is to undergo enzyme-linked immunosorbent assay (ELISA) testing for HIV. Which of the following information should the nurse include?
The test monitors the progression of the disease
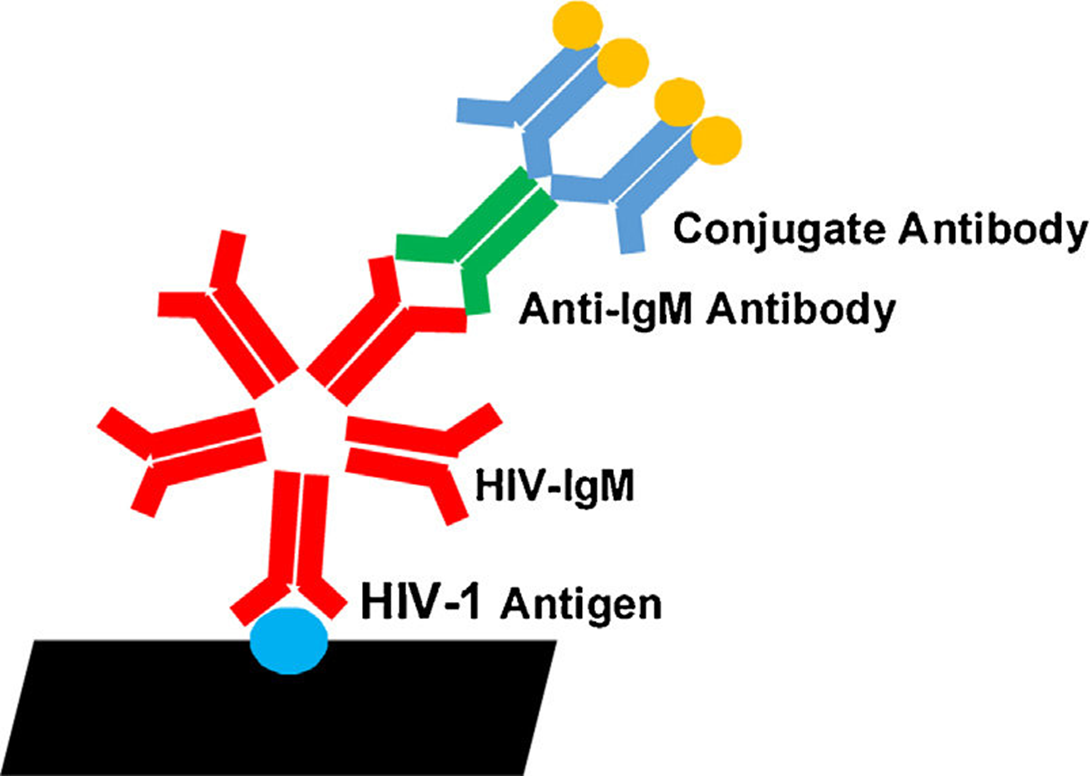
The test measures antibodies to the virus
The test results are accurate 24 hours after exposure to the virus
A positive result requires initiating immunoglobulin administration
The Correct Answer is B
Choice A reason: The test does not monitor the progression of the disease, as it only detects the presence of antibodies to HIV, not the amount of virus or the damage to the immune system. Other tests, such as viral load and CD4 count, are used to monitor the progression of HIV infection and the response to treatment.
Choice B reason: The test measures antibodies to the virus, which are produced by the immune system in response to HIV infection. The test is used to screen for HIV infection and to confirm the diagnosis. A positive result indicates that the person has been exposed to HIV and has developed antibodies to the virus.
Choice C reason: The test results are not accurate 24 hours after exposure to the virus, as it takes time for the body to produce enough antibodies to be detected by the test. The window period, which is the time between exposure to HIV and a positive test result, varies from person to person, but it can range from 3 weeks to 3 months. Therefore, a negative result does not necessarily rule out HIV infection, and a repeat test may be needed after the window period.
Choice D reason: A positive result does not require initiating immunoglobulin administration, as immunoglobulin is not a treatment for HIV infection. Immunoglobulin is a preparation of antibodies that can provide temporary protection against some infections, but it does not affect HIV. A positive result requires further confirmation by a more specific test, such as the Western blot, and referral to a specialist for treatment and counseling.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","D","E"]
Explanation
Choice A reason: Investigating potential health and environmental issues is a key function of community-oriented nursing, as it helps to identify and address the factors that affect the health of the population.
Choice B reason: Initiating support groups for parents of autistic children is not a specific task of community-oriented nursing, as it focuses on a particular subgroup rather than the whole population. This is more aligned with community-based nursing, which provides care to individuals and families in their natural settings.
Choice C reason: Providing wound care for clients in their homes is not a specific task of community-oriented nursing, as it focuses on individual needs rather than population needs. This is also more aligned with community-based nursing, which provides direct care to clients in their homes.
Choice D reason: Participating in local health surveillance activities is a key function of community-oriented nursing, as it helps to monitor and evaluate the health status and trends of the population.
Choice E reason: Providing health-related education to community groups is a key function of community-oriented nursing, as it helps to promote health and prevent disease among the population.
Correct Answer is B
Explanation
Choice A reason: A humidifier should be placed beside the child's bed is not the information that the nurse should include, as it is not relevant to pertussis. Pertussis, or whooping cough, is a bacterial infection that causes severe coughing spells, difficulty breathing, and a characteristic whooping sound. A humidifier may help with other respiratory conditions, such as bronchitis or asthma, but it does not affect pertussis.
Choice B reason: Household contacts will receive prophylactic antibiotics is the information that the nurse should include, as it is an important measure to prevent the spread of pertussis. Pertussis is highly contagious and can be transmitted through respiratory droplets from coughing or sneezing. Household contacts, especially those who are not fully vaccinated or have a weakened immune system, are at risk of contracting pertussis from the child. Prophylactic antibiotics, such as azithromycin or erythromycin, can reduce the risk of infection and complications.
Choice C reason: Transmission will be prevented because of herd immunity is not the information that the nurse should include, as it is not true for pertussis. Herd immunity is the protection that occurs when a large proportion of the population is immune to a disease, either through vaccination or natural infection. Herd immunity can reduce the transmission of some diseases, such as measles or polio, but it is not effective for pertussis. This is because pertussis immunity wanes over time, and the current vaccines do not provide long-lasting protection. Therefore, even vaccinated people can get or spread pertussis.
Choice D reason: The child is most contagious after the rash develops is not the information that the nurse should include, as it is not true for pertussis. Pertussis does not cause a rash, unlike some other childhood diseases, such as measles or chickenpox. The child is most contagious during the first two weeks of the illness, when the symptoms are similar to a common cold. The coughing spells usually start after the first week and can last for several weeks or months.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today