A nurse is planning care for an older adult client who has herpes zoster. Which of the following interventions should the nurse include in the plan?
Administer analgesics for pain
Restrict visitors who have hot previously received a measles, mumps, and rubella vaccine.
Place the client in protective isolation.
Avoid the use of alcohol-based hand rubs.
The Correct Answer is A
Choice A rationale: Pain management is a crucial aspect of care for a client with herpes zoster (shingles). Administering analgesics can help alleviate pain and improve the client's overall comfort.
Choice B rationale: Herpes zoster is not spread through respiratory droplets, so restricting visitors based on their vaccination status is not necessary.
Choice C rationale: Protective isolation is not required for herpes zoster, as it is not highly contagious.
Choice D rationale: There is no need to avoid alcohol-based hand rubs in the care of a client with herpes zoster.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is ["A","C","D"]
Explanation
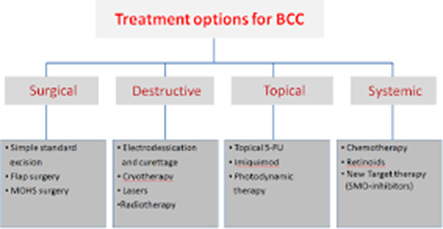
Choice A rationale: radiation therapy is one of the possible management options for basal cell carcinoma (BCC) that uses high-energy rays to kill the cancerous cells.
Choice B rationale: this is incorrect since topical corticosteroids are ineffective in BCC management and may worsen the patient’s condition by suppressing their immune system.
Choice C rationale: micrographic surgery can be used in BCC management and it involves the removal of thin layers of skin to a point where no cancer cells can be detected.
Choice D rationale: this is appropriate and involves the use of electric current to burn off the cancer cells.
Correct Answer is ["325"]
Explanation
In burns, half the total fluids required within 24 hours should be given within 8 hours and the other half distributed over the remaining 16 hours to prevent hypovolemic shock and electrolyte imbalance.
Therefore, half the fluid that should be given within 8 hours is 5200/2= 2600
We will use the formula: drip rate= total volume of fluid to be administered/total duration
= 2600/8
=325 mL/hr
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today