A nurse is preparing to administer several medications to a client. Which of the following data should the nurse plan to use to confirm the client's identity?
The client's room number
The client's admitting diagnosis
The name of the client's next of kin
The client's telephone number
The Correct Answer is D
The nurse should plan to use the client's telephone number to confirm their identity. This is because the telephone number is a unique identifier that is directly associated with the client and can be easily verified. By comparing the client's telephone number with the information on the medication administration record or electronic health record, the nurse can ensure that the right medication is given to the right patient.
Explanation:
a) The client's room number is not a reliable method to confirm the client's identity because multiple clients may be assigned to the same room, and there is a possibility of room changes or transfers.
b) The client's admitting diagnosis is not a suitable method to confirm identity as it does not provide specific information about the individual patient.
c) The name of the client's next of kin is not a reliable method to confirm the client's identity as it refers to a family member or emergency contact, not the client themselves. Additionally, next of kin information may not always be up to date or readily available.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is A
Explanation
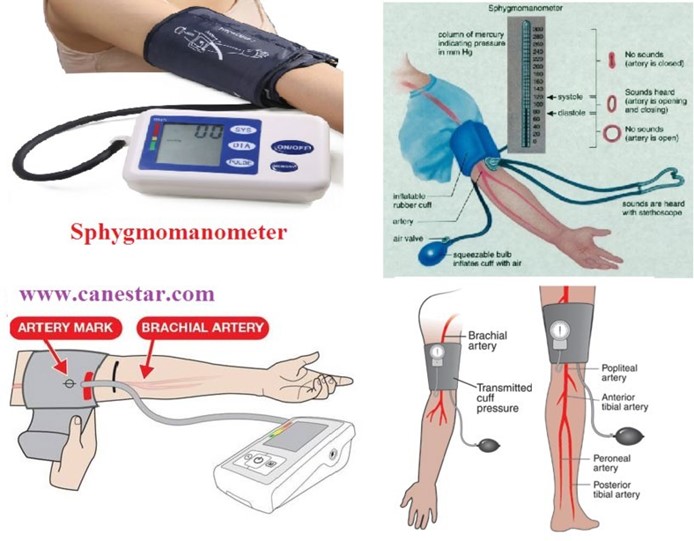
When checking a client's blood pressure, the nurse should use a cuff with a width that is about 60% of the client's arm circumference. This will help to ensure that the cuff fits properly and provides an accurate reading.
Options b, c, and d are not correct. The cuff should be applied over the client's brachial artery, which is located in the antecubital fossa. The client should sit with their arm resting at the level of their heart, not above it. The pressure on the client's arm should be released at a rate of 2 to 3 mm per second, not 5 to 6 mm per second.
Correct Answer is C
Explanation
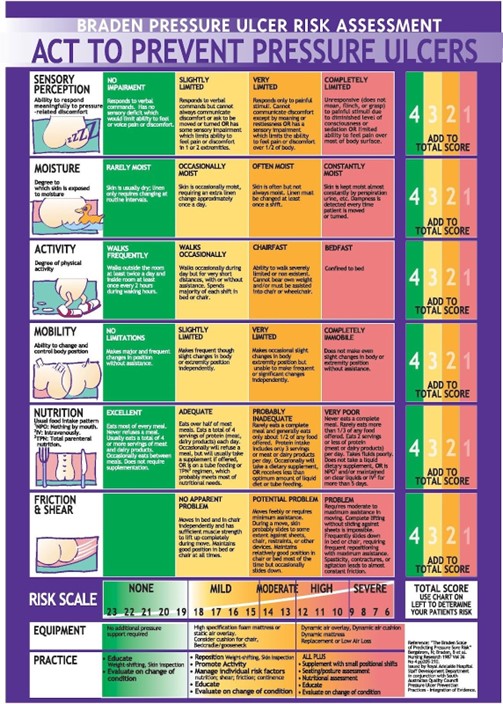
The Braden scale measures six elements: sensory perception, moisture, activity, mobility, nutrition, and friction/shear. Each element has a range of one to four points, with a total possible score of 23 points. The lower the score, the higher the risk for pressure injury.
Option a is incorrect because each element has a range from one to four points.
Option b is incorrect because the lower the score, the higher the pressure injury risk.
Option d is incorrect because the client's age is not part of the measurement.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today