A nurse is reinforcing teaching with a client about intermittent catheterization to measure residual urine. Which of the following information should the nurse include in the teaching?
"You cannot drink fluids for 4 hours after the procedure."
"You will need to urinate before the procedure."
"You will feel pressure when I inflate the catheter balloon."
"You will have a leg bag to collect the urine."
The Correct Answer is B
The correct answer is B. "You will need to urinate before the procedure." The rationale for this information is that intermittent catheterization is a method of draining urine from the bladder using a thin, flexible tube called a catheter. It is used to measure residual urine, which is the amount of urine left in the bladder after voiding. Residual urine can indicate problems with bladder function, such as obstruction, infection, or nerve damage .
To measure residual urine, the client should first empty their bladder by urinating normally. Then, the nurse will insert the catheter into the urethra and advance it into the bladder.The nurse will measure the amount of urine that drains out of the catheter and record it as residual urine. The nurse will then remove the catheter and dispose of it .
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is D
Explanation
The correct answer is D.
Iron absorption is inhibited by calcium, which is found in milk and dairy products. Therefore, the nurse should advise the client to avoid drinking milk with the iron supplement. The nurse should also encourage the client to consume foods rich in vitamin C, such as berries and citrus fruits, which can enhance iron absorption.
Correct Answer is D
Explanation
Choice A reason:
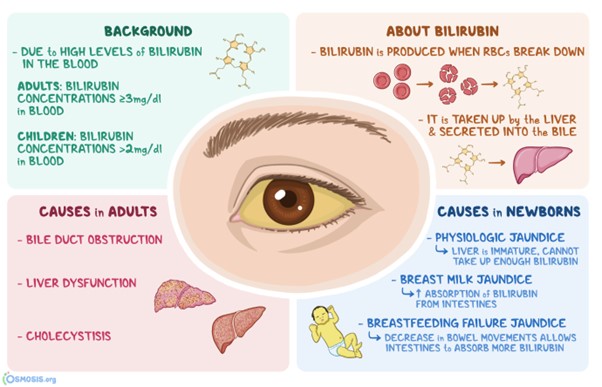
The face is incorrect: Facial skin colour can vary for many reasons, but it may not be the best indicator of jaundice in individuals with dark skin.
Choice B reason
Shoulders is incorrect: The shoulders are not typically indicative of jaundice.
Choice C reason:
Palm of the hands is incorrect: While the palm of the hands can sometimes show yellowing in cases of jaundice, it is less reliable than observing the sclera.
Choice D reason:
Sclera is the best location. In individuals with darker skin tones, yellowish discoloration of the skin due to jaundice can be more challenging to detect. However, the sclera of the eyes can still show noticeable yellowing, making it a reliable location for assessing jaundice in individuals with both light and dark skin.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today