A nurse is verifying informed consent for a client who is preoperative for a vaginal hysterectomy. Which of the following statements should the nurse identify as an indication that the client has given informed consent?
“I will have a large scar on my stomach after this procedure."
"I am thankful I am done having children."
"I should expect my periods to resume in 1 month."
"I will no longer need a regular gynecological examination."
The Correct Answer is B
Informed consent is a process where the healthcare provider explains the risks, benefits, and alternatives of a proposed procedure or treatment to the client. The client then demonstrates their understanding of this information and voluntarily agrees to undergo the procedure or treatment.
A. "I will have a large scar on my stomach after this procedure". This is incorrect for a vaginal hysterectomy, which does not involve an abdominal incision.
B. 'I am thankful I am done having children." This statement reflects an understanding of a key consequence of a hysterectomy, which is the removal of the uterus and the resulting inability to have children. This indicates that the client is aware of and accepts the major impact of the surgery on their reproductive capabilities.
C. "I should expect my periods to resume in 1 month.": This is incorrect because the removal of the uterus means the client will no longer have menstrual periods.
D. "I will no longer need a regular gynecological examination.": This is incorrect because regular gynecological examinations are still necessary to monitor overall reproductive health and screen for other conditions.
Nursing Test Bank
Naxlex Comprehensive Predictor Exams
Related Questions
Correct Answer is C
Explanation
Dependent personality disorder is characterized by an excessive reliance on others for decision-making and a fear of being alone or taking responsibility. Encouraging the client to be assertive helps promote their independence and self-confidence. It allows them to express their needs and preferences, make decisions, and take responsibility for their own actions. Empowering the client to be assertive can enhance their overall well-being and promote healthier relationships.
Limiting the client's social interactions may exacerbate their dependency and hinder their progress in developing more self-reliance and independent coping skills. It is important to encourage appropriate and healthy social interactions while also promoting the client's independence.
Maintaining a verbal no-harm contract with the client is a strategy more commonly used for clients at risk of self-harm or harm to others. It may not be directly applicable to the care of a client with dependent personality disorder unless there are specific safety concerns. Assuming responsibility for making the client's decisions would reinforce their dependency and enable their avoidance of taking personal responsibility. It is important to promote autonomy and support the client in making their own decisions whenever possible.
Correct Answer is ["C"]
Explanation
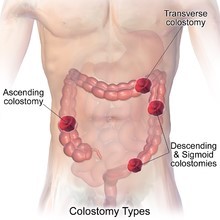
A. Create an opening on the skin barrier that is 1.27 cm (0.5 in) larger than the client's stoma.The opening on the skin barrier should be cut to fit closely around the stoma, approximately 0.3-0.6 cm (1/8 to 1/4 inch) larger than the stoma size. A larger opening (like 0.5 inches) could expose too much surrounding skin, increasing the risk of skin irritation from contact with the stoma's effluent.
B. Use a moisturizing soap to clean the skin around the client's stoma.Moisturizing soaps should be avoided because they can leave a residue on the skin, which may interfere with the adhesion of the ostomy appliance. The skin around the stoma should be cleaned with mild soap and water, or water alone, and then dried thoroughly before applying the new appliance.
C. Empty the client's ostomy pouch before removing the skin barrier.Emptying the ostomy pouch before removing the skin barrier is a practical step to reduce spillage of stool during the appliance change, making the process cleaner and easier to manage. It also minimizes the risk of contamination of the surrounding area or wound.
D. Change the client's ostomy appliance 1 hour after breakfast.Ostomy appliances are best changed when the bowel is least active, which is usually before a meal or several hours after eating. Changing the appliance shortly after a meal, such as 1 hour after breakfast, may result in more stoma output, making it harder to manage the appliance change.
Whether you are a student looking to ace your exams or a practicing nurse seeking to enhance your expertise , our nursing education contents will empower you with the confidence and competence to make a difference in the lives of patients and become a respected leader in the healthcare field.
Visit Naxlex, invest in your future and unlock endless possibilities with our unparalleled nursing education contents today